The molecular basis of inherited complement C3 deficiency in a 20-year-old newly diagnosed male patient was studied. Using an enzyme-linked immunosor-.
Eur. J. Immunol. 1994.24: 1517-1522
Yitzhak Katzo, Lon SingerA, Rick A. WetseP, Menachem Schlesingero and Zvi Fishelson. Unit of Allergy and Immunology and Department of Pediatrics, Assaf Harofeh Medical Center, Affiliated to the Sackler School of Medicine, Tel Aviv Universityo, Tel Aviv, Washington University School of Medicine, Children’s Hospital., St. Louis, Barzilai Medical Centero, Ashkelon and Department of Cell Biology and Histology, Sackler School of Medicine, Tel Aviv University., Tel Aviv
Inherited C3 deficiency
Inherited complement C3 deficiency: a defect in C3 secretion* The molecular basis of inherited complement C3 deficiency in a 20-year-old newly diagnosed male patient was studied. Using an enzyme-linked immunosorbent assay, the patient’s C3 serum level was found to be approximately 7 pg/ml, which is less than 1 % of normal. In contrast, Northern analysis indicated that the patient’s C3 mRNA was of normal size and quantity. Peripheral blood monocytes (PBM) and skin fibroblast cultures (F) from the patient and from healthy donors were labeled for 2 h with [”S] methionine. Analysis of cell lysates and supernatants by immunoprecipitation and sodium dodecyl sulfate-polyacrylamide gel electrophoresis (SDS-PAGE) demonstrated normal levels of C3 in lysates of patient’s PBM and F. However, C3 secretion in the patient’s cells was extremely reduced, with pulse-chase experiments demonstrating a long delay in the disappearance of intracellular C3. Secretion of C l r and factor B by the patient’s cells was normal. Lipopolysaccharide and interleukin-1 increased C3 synthesis in the patient’s PBM and F, but had no effect on the secretion. SDS-PAGE analysis of trypsin-cleaved intracellular C3 revealed an aberrant cleavage profile for the patient’s C3. Collectively, these data indicate that C3 deficiency in this patient is due to a defect in the C3 secretion, probably as the result of abnormality in the proC3 structure.
1 Introduction The third component of the complement system, C3, is the most abundant complement protein, has multiple binding sites to other proteins and is a source for biologically active fragments mediating immune adherence, phagocytosis and non-cytotoxic enzyme release, among many other complement reactions [l]. C3 is synthesized as a single-chain pre-pro-protein [2], pre-pro-C3, which is processed, glycosylated and secreted as a 180000 M, glycoprotein comprised of disulfide-linked a- and @-polypeptides with molecular weights of 115OOO and 70000, respectively. Inherited C3 deficiency has been described in 17 individuals from several families and shows an autosomal co-dominant pattern of inheritance [3]. Because of the numerous functions of C3 it is not surprising that individuals who are homozygously C3-deficient all suffer from either recurrent infections with pyogenic encapsulated bacteria [4], or various autoimmune disorders such as nephritis [5], lupus [6] and vasculitis [7] or both. The main source of C3 is the liver [8], but many extrahepatic sites were identified, including monocytes [9], fibroblasts [lo] and alveolar cells [ 111.There are differences in the amounts of circulating C3 in the sera of patients with C3 deficiency [12-141, and in some patients detectable amounts of C3 were synthesized by monocytes [15]. Recently, the molecular basis of C3
*
1517
deficiency in two patients was described. The first had a GT-AT splicer site mutation [16] and the second had a 800-bp gene deletion [17].We have analyzed monocytes and fibroblasts from a patient with a newly diagnosed C3 deficiency and found that the deficiency resulted from a defect in C3 secretion. The defect in secretion was accompanied by an abnormal pattern of trypsin digestion of the intracellular C3, suggesting an abnormality in the structure of the patient’s C3.
2 Materials and methods 2.1 Patient AGI was identified as having C3 deficiency during an episode of meningococcal meningitis. Blood serum samples collected on multiple occasions contained no detectable C3 protein and complement hemolytic activity (CH50). In addition, his serum contained antinuclear antibody. His past medical history was positive for several bacterial infections including periorbital cellulitis and pneumonia. The patient recovered without sequela. AGI was immunized with pneumococcal and meningococcal vaccines. The whole family was screened and C3 deficiency was found in a 7-year-old sister, whereas intermediatory low levels of C3 were found in the sera of both parents.The clinical details of AGI have been recently described [18].
[I 124471 The values for the levels of C3, CH50 and AP50 for the patients and family members are as shown in Table 1.
This work was supported by a Research Grant (1557) from the Chief Scientist, Ministry of Health, Israel (Y.K.), and NIH Grants A125011 and A100919 (R.A.W.).
Correspondence: Yitzhak Katz, Allergy and Immunology Unit, Assaf Harofeh Medical Center, Zerifin 70300, Israel Key words: Complement I C3 I Deficiency I Secretion 0 VCH Verlagsgesellschaft mbH, D-69451 Weinheim, 1994
2.2 Cells Human fibroblast lines were developed in our laboratory. Biopsies were obtained from the forearm of a patient with C3 deficiency (AGI) and four normal donors (9, 17,23 and 0014-2980/94/0707-1517$10.00+ .2510
1518
Eur. J. Immunol. 1994.24: 1517-1522
Y. Katz, L. Singer, R. A.Wetsel et al.
Table 1. Levels of C3 and functional complement activity in AGI and family members
c3
AGI(patient) AVG(sister) ANG(sister) KEN(father) OFG(mother) Normal Pooled serum
mg/100 ml
CH50 U/ml
AP50 U/ml
Undetectable Undetectable
< 200 < 200
< 20 < 20
165 68 47 130 140
1265 976 925 1450 1370
146 106 60 181 140
42 years old, respectively), and fibroblast cell lines were established according to published methods [19]. Fibroblasts from passages 2-8 were used. Monocytes were prepared and cultured as previously described [14]. 2.3 Reagents DMEM, DMEM without methionine, trypsin, penicillinstreptomycin, L-glutamine, crystallized trypsin, soybean trypsin inhibitor and fetal calf serum were purchased from Biological Industries (Bet Haemek, Israel). L-['%] Methionine (sp. act. lo00 CUmmol) was purchased from Amersham (Buckinghamshire, GB). Autofluor was purchased from National Diagnostics (Manville, NJ). Goat polyclonal antibodies to human Clr, Cls, C1 inhibitor, C3, C4, C5 and factors B, H and I were purchased from Atlantic Antibodies (Scarborough, ME) and antibodies to human C2 from ICN Biochemicals Inc. (Irvine, CA). Formalin-fixed Staphylococcus aureus (immunoprecipitin) was purchased from Bethesda Research Laboratories, Life Technologies, Inc. (Gaithersburg, MD). Trans-epoxy succinyl-1-leucyl amido(4-guanidino) butane (E-64), bovine serum albumin, leupeptin, and molecular weight markers were obtained from Sigma, and sodium dodecyl sulfate (SDS), acrylamide, bis-acrylamide, deoxycholate, ammonium persulfate, TEMED, Tris and glycine were purchased from United States Biochemicals Corp. (USB; Cleveland, OH). Recombinant IL-la was a generous gift from Dr. Peter Lomedico (Hoffmann-La Roche Inc., Nutley, NJ). 2.4 ELISA Antigenic serum concentration of C3 was measured using an ELISA. The IgG fraction of goat anti-human C3 antibody (Atlantic Antibody) or a monoclonal antibody specific for C3a (Quidel, San Diego, CA) at 10 pg/ml and 100 pg/ml, respectively, in carbonate buffer, pH 9.6, was coated on wells of polystyrene microtiter plates (0.1 muwell) overnight at 37 "C. The plates were washed, then incubated with sera (0.1 muwell), diluted in PBS (pH 7.4), 0.05 YO Tween-20,O. 1 YO BSA for 2 h at 37"C.The plates were washed and incubated with 4 pg/ml (0.1 muwell) polyclonal goat anti-human C3 conjugated to horseradish peroxidase for 2 h at 37 "C.Plates were washed, then incubated with 0.2 ml of 0.33 mg/ml o-phenylenediamine in 0.1 M citric acid, 0.2 M dibasicsodium phosphate at room temperature until a color change was observed.The
peroxidase reaction was blocked with 4 M H2S04 (50 puwell). Calibrator 4 (Atlantic Antibody) was used to calibrate the assay; C3-depleted human serum (Quidel) was used as a negative control. 2.5 Cell cultures, biosynthetic labeling and immunoprecipitation Fibroblasts were grown to confluence in multi-well tissue culture plates in medium containing 10 % FCS, washed to remove serum and spent medium, and cultured for 16-24 h in DMEM with 1 mg/ml BSA alone (control) or in medium containing BSA and various concentrations of IL-1. Biosynthetic experiments were performed by incubating the cells for 2 h in methionine-free DMEM containing [35S]methionine (300 pCi/ml) as described [18]. Total protein synthesis was estimated from incorporation of methionine into TCA-insoluble protein. Cell lysates and extracellular medium were prepared for immunoprecipitation, preabsorbed, and then immunoprecipitated with formalin-fixed S. aurew. Immunoprecipitates were subjected to SDS-PAGE, and the gels were fixed, impregnated with autofluor, dried and exposed at - 70°C to X-ray film. Incorporation of [35S] methionine into the individual immunoprecipitated proteins was determined in gel slices after digestion with 15 YO hydrogen peroxide for 16 h at 65 "C and addition of ultima gold (Packard, Downers Grove, IL). Effects of the stimuli on protein synthesis were determined after correcting the specific protein counts in the gel slices for total protein synthesized in each sample. 2.6 Isolation of RNA and Northern blot analysis Normal fibroblasts and fibroblasts from patient AGI were grown to confluence in 162-cm2flasks and stimulated with IL-l(l0 ng/ml) 20 h prior to RNA harvest. Approximately 108 cells were lysed and RNA was harvested using the method described by Chirgwin et al. [20]. RNA was quantitated by absorbance at 260 nm. Polyadenylated mRNA was separated on an oligo(dT) cellulose column (Collaborative Research Products, Bedford, MA) using previously described methods [21]. Approximately 2 pg/ml poly(A)+ RNA was denatured and subjected to electrophoresis in a 1YO agarose/formaldehyde gel; the RNA was transferred to a nylon membrane (Amersham Life Sciences, Arlington Heights, IL) and processed as described by Vicra et al. [22]. The nylon-bound mRNA was hybridized to a nick-translated 32P-labeled 1-kb cDNA coding for the Bst EII fragment of the C3 gene pC3.59 [23]. The cDNA probe for actin was pAC269 [24].
3 Results 3.1 Detection of serum C3 by ELISA Using the IgG fraction of a monospecific polyclonal anti-human C3 antibody, with a sensitivity of 10 ng/ml, we have determined that this patient's serum contains approximately 7 pg/ml C3, which is less than 1 YO of the normal amount. These results were confirmed by a second ELISA using a monoclonal antibody to the C3a portion of the C3 molecule.
Eur. J. Immunol. 1994. 24: 1517-1522
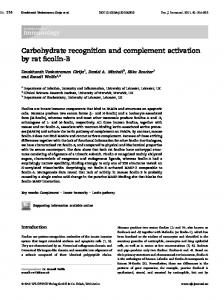
3.2 Detection of C3 mRNA by Northern blot analysis Twice selected poly(A)+ RNA was prepared from normal and AGI IL-1-stimulated fibroblasts, and the C3 and actin mRNA were analyzed by Northern blot analysis. The amount of C3 message in the two fibroblast cell types was subsequently compared by normalizing to the actin signal. The C3-specific message detected in the AGI fibroblasts was similar in size and quantity to the C3 message of normal fibroblasts (Fig. 1).
285-
-
Inherited C3 deficiency '11
(XlU-'r
ZUS -
117-
96-
66-
45-
c3
IC
-
LPS
IC
IC
IC
+
-
Normal
+
AG I
Figure 2. C3 synthesis in monocytes. Autoradiography of immunoprecipitates of intracellular (IC) lysates subjected to SDS-PAGE are shown. Monocyte monolayers from a normal donor and the C3-deficient patient (AGI) were incubated in medium alone (LPS-) or in medium containing LPS 1 pglml (LPS+) for 24 h and then labeled with [35S]methionine 300 pCi/ml for 120 min. At the end of the pulse period, the monolayers were rinsed and lysed in the presence of enzyme inhibitors. The lysates were immunoprecipitated with monospecific anti-C3 antibody.
185-
28s -
c3
Normal 18s- I
1519
+Actin
Factor B Normal AGI
AGI
--.
2051'17 96 66
Figure 1. Detection of C3 mRNA in AGI fibroblasts by Northern blot analysis. Twice selected poly(A)+ RNA was prepared from normal (N) and AGI IL-1-stimulated fibroblasts and the C3 and actin mRNA were analyzed by Northern blot analysis [l @ l a n e , with 9-h (C3) or 3 0 4 1 1 (Actin) exposure]. The amount of the message in the two fibroblast cell types was subsequently compared by normalizing to the actin signal.
3.3 C3 synthesis in monocytes The results of biosynthetic labeling and immunoprecipitation of C3 in monocytes from a normal donor and the patient (AGI) are shown in Fig. 2. Comparable amounts of newly synthesized intracellular C3 were demonstrated in monocytes of the patient and of the normal donor. No secreted C3 was detected in the medium recovered from the patient's cells during the 2-h pulse period (not shown). Incubation of the monocytes in medium containing LPS 1 p.g/ml, resulted in increased synthesis of proC3, both in cells of the patient and of the normal donor (Fig. 2). The secretion of other proteins of the complement system, such as C2,factor B, Clr, C l s and C1 inhibitor was normal in the same samples (data not shown). 3.4 C3 synthesis in fibroblasts To exclude the possibility that the defect in the secretion of C3 was confined to one cell type, we examined the synthesis
45
-.
-
1 2 3 4 5 6 7 6 IC EC IC Ec IC Ec IC EC
11-1d
-
- + + - -
+ +
1 2 3 4 5 6 7 6
IC Ec IC EC IC Ec IC EC
- -
+
+
-
-
+
+
Figure 3. C3 and factor B synthesis in fibroblasts. Autoradiography of SDS-PAGE analysis of C3 and factor B in skin-derived fibroblasts from a normal donor and from the C3-deficient patient (AGI). Confluent monolayers were incubated in medium alone or in medium supplemented with IL-1, 0.1 ng/ml, for 16 h and then biosynthetically labeled and analyzed as described in Sect. 2.5. IC: intracellular. EC: extracellular.
and secretion of complement proteins in fibroblasts from the patient and two normal donors. A representative experiment is shown in Fig. 3. AGI fibroblasts failed t o secrete C3 protein during the 2-h pulse period. In other aspects, synthesis and secretion of factor B and response to stimulation with I L l a , both cell types were comparable. Comparable amounts of Clr, Cls, C1 inhibitor and factor H were also detected in the medium recovered from the patient's and control fibroblasts (data not shown). The apparent molecular weight of the single-chain C3 precursor in AGI and normal cells was similar. One difference was observed in the structure of C3 between cell lysates of normal donor and AGI. In the former, two bands, corresponding to the a and p-chains of C3 were observed.These
1520
Eur. J. Immunol. 1994. 24: 1517-1522
Y. Katz, L. Singer, R. A. Wetsel et al.
bands, representing intracellular processing of the precursor C3 prior to the secretion, were not observed in fibroblasts derived from AGI (Figs. 2 and 3).
cells was estimated from pulse-chase experiments and two 24-h pulse experiments (Fig. 5). I n these experiments, the amounts of C3 in the medium of normal and AGI cells were compared with each other and normalized to amounts of
The rate of secretion of C3 from the normal and AGI fibroblasts was determined by quantitation of the amount of C3 protein at the various time points of the pulse-chase experiment, such as the one shown in Fig. 4. ,The disappearance of intracellular C3 from AGI cells was considerably slower than from normal cells. For example, 3 h after completion of the pulse, only 6 % of proC3 remained in the lysates of normal cells, while near starting levels of C3 remained in AGI cells (Fig. 4 and Table 2). Furthermore, only small amounts of secreted C3 were detected in the extracellular medium of the AGI cells 8-20 h after completion of the pulse. Precursor C3 was secreted from the normal and AGI fibroblasts in parallel to the secretion of a and p chains (Figs. 3-5). The extracellular a and p chains in AGI cells had an apparent molecular size similar to that of normal C3. The SDS-PAGE band of intracellular fi chain of AGI fibroblasts pulsed for 24 h appeared slightly higher than that of normal p chain (Fig. 5).The total amount of C3 secreted from AGI
A
96 A6
45
1
::I
Foctor B 1
2 3 4 5 6 7 8 9 1 0 1 1
1
3
4
EC
5
6 IC
7
8 EC
Figure 5. Synthesis and secretion of C3 and factor B by fibroblasts labeled for 24 h. Autoradiograms of SDS-PAGE analysis of immunoprecipitated C3 (lanes 1-4) and factor B (lanes 5-8) synthesized in skin-derived fibroblasts from AGI (lanes 1, 3, 5, 7) and a normal donor (lanes 2, 4, 6, 8). Fibroblasts were pretreated for 20 h with IL-la (10 nglml), biosynthetically labeled for 24 h and analyzed as described in Sect. 2.5. IC: intracellular, EC: extracellular.
i:::I c[
2
IC
AGI
0.
Normal
117
2 3 4 S L 7 8 9 1 0 1 1
Figure 4. Rate of secretion of C3 and factor B from normal and AGI fibroblasts. Fibroblasts were metabolically labeled as described in Sect. 2.5, washed and incubated in medium containing excess unlabeled methionine for the times indicated, up to 20 h. The intracellular lysates (IC) and extracellular medium (EC) were immunoprecipitated with antibodies to C3 or factor B. Lane 1: Proteins immunoprecipitated from the extracellular medium after 2-h pulse, (repre-
Table 2. Rate of disappearance of complement proteins from normal and AGI fibroblastsa)
Factor B
c3
Hours post pulse
Clr
N
AGI
N
AGI
N
AGI
0
100
100
100
100
100
100
1
61.6 (59.4-66.8)
90.7 (84.6-93.2)
66.6 (58.4-72.3)
63.8 (53.1-70.3)
40.3 (33.7-54.1)
31.4 (26.7-36.1)
3
5.8 (2.1-7.6)
107.3b) (90.3-1 10.3)
10.2 (8.4-17.3)
13.5 (9.3-16.4)
11.6 (9.1-13.3)
8C)
3.2 (1.6-4.8)
60.2 (48.3-72.1)
7.8 (5.1-10.5)
13.3 (9.6-16.4) 8.1 (6.8-9.4)
6.3 (4.7-7.9)
20
0
6.3 (3.4-12.1)
5.3 (3.1-6.8)
7.8 (4.1-9.3)
0
7.4 (5.2-9.6) 0
a) Data from three different pulse-chase experiments presented as percent of protein detected in cell lysates (intracellular), as calculated from cutting the appropriate slices from the gel, digestion and counting in a p-counter. Mean and range are indicated. b) Percent residual C3 at this time point is above the 100% level since there was continuous synthesis of C3. after termination of the pulse methionine. utilizing the excess intracellular radiolabeled [35S] c) Data from tw o experiments only.
Eur. J. Immunol. 1994. 24: 1517-1522
other proteins of the complement system, such as factor B and Clr, that were secreted. From these experiments we estimated that the secretion of C3 from AGI cells was approximately 8 % of that expected (Figs. 4 and 5).
3.6 %sin
digestion of intracellular C3
The result of digestion of intracellular C3 with trypsin is shown in Fig. 6. Extracts of metabolically labeled normal and AGI fibroblasts were treated for 10 min at room temperature with trypsin at 2.0 mg/ml. The reaction was terminated by addition of soybean trypsin inhibitor and the resultant fragments were immunoprecipitated with anti-C3 antibodies and analyzed by SDS-PAGE. The lysates of the normal cells contained two major bands of 105 and 70 kDa. The lysates of AGI cells contained three bands with apparent molecular mass of 105, 97 and 75 kDa, but the principal fragment of 70 kDa was not detected (Fig. 6). When the lysates were treated with lower concentration of trypsin, 0.2 or l.Omg/ml, partial digestion of C3 was observed in both cell types, suggesting that the sensitivity of the single-chain precursor C3 to digestion by trypsin was similar in AGI and in normal fibroblasts (data not shown).
205-
116-
97-
Inherited C3 deficiency
1521
delayed and incomplete and, even after the complete disappearance of the intracellular C3, only a small amount of intracellular C3 was recovered from the extracellular medium. AGI fibroblasts secreted approximately 8 % of the amount of C3 secreted by normal cells over a period 20 h; however the serum level of C3 in AGI was only about 1% of normal. This discrepancy has at least two explanations; the first being that the major source of serum C3 is not fibroblasts but rather the liver [8], and the second is that the serum C3 level reflects a balance between synthesis and consumption. No gross abnormality was detected in AGI with respect to the size of C3 mRNA or precursor C3 protein. More precursor C3 was found intracellularly in AGI than normal fibroblasts. However, analysis of the intracellular processing of C3 has suggested some abnormality on the protein level (Fig. 5, lane 1). Surprisingly, extracellular C3 in AGI appears to have normal-sized a and fi chains (Fig. 5, lane 3). Trypsin digestion studies have also indicated that the single-chain precursor C3 in AGI has a structural abnormality. Treatment of the intracellular C3 of normal fibroblasts with trypsin, produced two major bands of 105 and 70 kDa (Fig. 6). It is likely that the precursor C3 was cleaved first to C3, comprised of the 115 kDa a chain and the 70 kDa fi chain. Next, trypsin probably cleaved the a chain of C3 to the a' chain of 105 kDa [23,25]. In contrast, cleavage of the precursor C3 of AGI resulted in generation of 105-, 97- and 75-kDa fragments.The 105-kDa band may perhaps be an a' chain of the AGI C3. However, it is not yet clear what the other two bands are. One possibility is that they are fragments of the achain, although the 75-kDa band could be an abnormal fi chain, migrating for some reason more slowly than a normal fi chain.
Taken together, these results raise the following possibilities: normally, as soon as the proC3 is processed into C3, the protein is secreted from the cell [26]. Some proC3 may be 66secreted (at least in vitro) without processing (Figs. 3 and 4). Due to its abnormal structure, the proC3 of AGI is processed much slower into C3, and is, therefore, not N N AGI secreted but rather accumulated inside the cells. The EC IC IC abnormal proC3 of AGI is possibly cleaved intracellularly by a trypsin-like enzyme and is eventually (after 10-20 h) + + Trypa i n completely digested (Figs. 5 and 6). The small fraction of Figure6. Trypsin digestion of proC3 in normal and AGI fibro- proC3 in AGI which is processed at a slower rate into blasts. Fibroblast monolayers were metabolically labeled and the normal C3, is immediately secreted from the cells.This may intracellular lysates were incubated with 2.0 mg/ml trypsin for explain the presence of C3 a and fi chains in the extracel10 min at 37"C.The reaction was terminated with soybean trypsin Ma r medium of AGI fibroblasts. Alternatively, released inhibitor and the resultant fragments were immunoprecipitated proC3 may be cleaved extracellularly by ecto-proteases into with polyclonal anti-human C3 antibody and analyzed by SDS- apparently normal C3. Another possible explanation is that PAGE. Left lane: extracellular medium from normal fibroblasts without treatment with trypsin (shown for orientation). Center AGI may contain two distinct abnormal genes, one encodlane: intracellularlysate from normal fibroblasts and the right lane: ing a protein which is completely degraded intracellularly intracellular lysate from AGI fibroblasts, both after trypsin and a second encoding a protein which is processed normally but at a reduced rate. digestion.
4 Discussion We report here of a novel type of C3 deficiency, manifested by normal levels of intracellular C3, but extremely reduced amounts of secreted protein. The secretion of C3 was
Molecular analysis of cDNA prepared from the mRNA of AGI fibroblasts, revealed a nucleotide substitution in the C3 gene from AGI which results in a single amino acid substitution in the fi chain at residue 549 (Asp to Asn) [27]. This amino acid change in the proC3 may cause incomplete processing, and intracellular degradation of proC3 (Fig. 6).
1522
Eur. J. Immunol. 1994. 24: 1517-1522
Y. Katz, L. Singer, R. A.Wetsel et al.
Transfection and PCR experiments are currently underway to determine if this amino acid substitution causes the secretory impairment and if it is contained in both C3 alleles of this C3D kindred.
5 References
1 Fishelson, Z., Mol. Immunol. 1991. 28: 545. 2 Brade,V., Hall, R. E. and Colten, H. R., J. Exp. Med. 1977. 146: 759. 3 Morgan, B. P. and Walport, M. J., Immunol.Today 1991. 12: Patients with C3 deficiency have an increased incidence of 301. infections andor features of autoimmune phenomena 4 Alper, C. A., Colten, H. R., Rosen, F. S., Rabson, A. R.. [3-61. Our patient expressed symptoms similar to other Macnab, G. M. and Gear, J. S. S., Lancet 1972. ii: 1179. C3-deficient patients. He suffered several times from 5 Pussell, B. A., Bourke, E., Nayef, M., Morris, S. and Peters, pyogenic infections and arthralgia with elevated antinuD. K., Lancet 1980. i: 675. clear factor; both types of defects had relatively mild 6 Sano,Y., Nishimukai, H., Kitamura, H., Nagaki, K., Inai, S.. Hamasaki,Y., Maruyama, I. and Igata, A., Arthritis Rheum. expression. Neither the infections nor the autoimmune 1981. 24: 1255. phenomena resulted in serious restriction of normal life 7 Strate, M., Olsen, H. and Teisner, B., Eur. J. Clin. Invest. 1987. style. It may be that the low C3 level found in the 17: 226. circulation of this patient contributes to his relative resisAlper, C. A., Johnson, A.M., Bistch, A. G. and Moore, 8 tance to disease. R. D., Science 1969. 163: 286. 9 Einstein, L. P., Hanson, P.,Ballow, M., Davis, E., Davis, J. S., Our data, together with that already published, suggest Alper, C. A., Rosen, F. S. and Colten, H. R., J. Clin. Invest. that human C3 deficiency is caused by a heterogenous array 1977. 60: 963. of molecular defects. For example, two C3-deficient 10 Katz,Y. and Strunk, R. C., Arthritis Rheum. 1988. 31: 1365. patients that have been studied at the molecular genetic 11 Strunk, R. C., Eilden, D. M. and Mason, R. J., J. Cfin. Invest. 1988. 81: 1419. level, each exhibit a different mutation [16, 17].The C3 null gene of one patient contained a G T to AT mutation at the 12 Kitamura, H., Nishimukai, H. and San0.Y. and Nagaki. K., Immunology 1984. 51: 239. 5' donor splice site of intron 18. This mutation caused a 13 Davis, A. E. 111, Davis, J. S. IY Rabson, R. A., Osofsky, 61-bp deletion in the C3 mRNA by splicing a cryptic S. G., Colton, H. R., Rosen, F. S. and Alper, C. A.. Clin. 5' donor splice site in exon 18 with the normal 3' splice site Immunol. Immunopathol. 1977. 8: 543. in exon 19.The C3 gene of the second patient contained an 14 Alper, C. A., Propp, R. P., Klemperer. M. R. and Rosen. F. S.. 800-bp deletion that included exons22 and 23. Both of J. Clin. Invest. 1969. 48: 553. these mutations cause a reading frame shift so that 15 Einstein, L. P., Hansen, P. J., Ballow, M., Davis, A. E. 111, Davis, J. S. IV, Alper, C. A., Rosen, F. S. and Colten, H. R., J. biosynthesis of normal size C3 could not occur.The patient Clin. Invest. 1977. 60: 963. studied in this report clearly has a different molecular genetic defect, since normal size C3 mRNA and proprotein 16 Botto, M., Fong, K. Y., So, A. K., Rudge, A. and Walport, M. J., J. Clin. Invest. 1990. 86: 1158. were produced in normal quantities in the deficient cells. In Botto, M., Fong, K. Y., So, A. K.. Barlow, R., Routier, R.. addition, we are also studying a C3-deficient patient of 17 Morley, B. J. and Walport, M. J., Proc. Natl. Acad. Sci. USA Laotion decent that synthesizes normal-size C3 mRNA and 1992. 89: 4957. proprotein, but in contrast to the AGI cells, this patient's 18 Peleg, D., Harit-Bustan, H., Katz,Y., Peller. S., Schlesinger, M. cells have reduced amounts of C3 mRNA and proprotein and Schonfeld, S.. Pediatr. Infect. Dis. 1992. 11: 401. [28]. Thus, these four patients have distinct molecular 19 Katz,Y., Cole, F. S. and Strunk, R. C.,J. Exp. Med. 1988. 167: 1. mutations each causing C3 deficiency. 20 Chirgwin, J. M., Przybyla, A. E., MacDonald, R. J. and Rutter, W. J., Biochemistry 1979. 18: 5294. In conclusion, complement C3 deficiency in the patient 21 Saiki, R. K., Gelfand, D. H., Stoffel, S., Scharf, S. J., Higuchi, reported here is caused by a defect in C3 secretion, R., Horn, G. T., Mullis, K. B. and Erlich, H. A., Science 1988. probably as the result of an abnormality in the C3 structure. 239: 486. A very similar RNA and protein phenotype has recently 22 Virca, D. D., Northemann, W., Shiels, B. R.. Widera, G. and been described for type I1 C2 deficiency; cells from a type I1 Broome, S., Biotechniques 1990. 8: 370. CZdeficient patient had normal amounts of C2 mRNA and 23 De Bruijn, M. H. L. and Fey, G. H.. Proc. Natl. Acad. Sci. intracellular protein but secreted only a limited amount of USA 1985. 82: 708. C2 [29]. Elucidation of the molecular genetic mutations 24 Schwartz, R. J., Haron, J. A., Rothblum, K. N. and Dugaiczyk, A., Biochemistry 1980. 19: 5883. causing C2 and C3 deficiencies of this kind should yield insights into structural abnormalities in protein molecules 25 Alsenz, J., Becherer, J. D., Nilsson, B. and Lambris, J. D., Curr. Top. Microhiol. Immunol. 1990. 153: 235. that result in cellular secretory defects in general. 26 Barnum, S. R., Fey, G. and Tack, B. F., Curr. Top. Microhiol. Immunol. 1989. 153: 23. 27 Singer, L., Katz,Y., Schlesinger, M., Fishelson, Z. and Wetsel. We would like to thank Dr. D. Peleg for referring the patient to us, R. A., Mol. Immunol. 1993. 30: (Suppl I ) : 51. I? Koch for skilled technical support, and Anji Agajany and Jane 28 Singer, L.. Kramer, J., Borzy, M. S. and Wetsel, R. A., Compl. Geva for their expert secretarial assistance. Inflamm. 1991. 8: 274. 29 Johnson, C. A., Densen, P.,Wetsel, R. A., Cole, F. S., Goeken, Received October 15. 1993; in revised form March 21, 1994; N. E. and Colten, H. R., N. Engl. J. Med. 1992. 326: 870. accepted March 24. 1994.