Mar 30, 1992 - Robotic Chromatography: Development and Evaluation of Automated Instrumentation .... We wrote custom-designed software for the Hamilton.
CLIN. CHEM. 39/1, 143-147 (1993)
Robotic Chromatography: Development and Evaluation of Automated Instrumentation for Assay of Glycohemoglobin Christopher D. Herold,’ Kirk Andree,2 David A. Herold,3’4 and Robin A. Felder’ The measurement
of glycohemoglobin
(GHb) by boronate
affinitychromatographyis usefulin monitoringlong-term glucose control in diabetic subjects. The inherent disadvantage of this method is the hands-on time required because the hemoglobin fractions are separated on individual disposable columns. To overcome this disadvantage, we have programmed a Hamilton Microlab 2200 automated pipetting cartesian robot to complete the procedure, from the aspiration of blood from the samplecollection tube to the transfer of the separated hemoglobin fractions to a microtiter plate for absorbance measurement. This automated robotic system can analyze 96 specimens, including patients’ samples and control material, in -3 h. The precision (CV) of the method ranged from 1.6% to 3.5% within-run and from 2.7% to 3.5% day-to-day. The results correlated with those obtained with the Accuflex semiautomated robot, which used the identical disposable column, and those obtained with a Primus high-performance liquid chromatograph, which used a regenerated microparticlecolumn. Automation of the GHb procedure allowed improved throughput, reduced labor cost, improved precision, and offered greater laboratory safety.
tively, a batch automated pipetting station can be programmed to manipulate disposable phenylboromc acid chromatography columns. Programmable devices to allow the automation of many labor-intensive tests, e.g., cartesian robots equipped for pipetting, have recently become available. These automated pipetting stations can be configured to perform many different fluid-handling tasks. Moreover, as analytical methods change in the laboratory, the pipetting station can be quickly reprogrammed, obviating the need to purchase additional equipment. Use of programmable laboratory automation such as pipetting stations and robotic arms has the potential to improve productivity, increase analytical flexibility, and offer greater safety from contaminated specimens. In this study, we used an automatic pipetting station with a custom-designed chromatographic-column holder to automate the boronate affinity minicolumn method for Glib. We then compared this method with the Accuflex pipetting station and the Prinius HPLC methods.
being free from many of the interferences
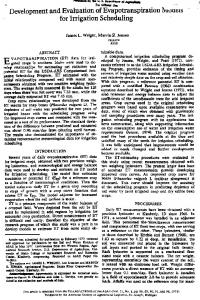
MaterIals and Methods Pipetting Stations The Microlab 2200 (Hamilton Co., Reno, NV), a programmable cartesian robot, allows a Teflon-coated pipette probe to move in space with x-, y-, and z-directional freedom. Figure 1 shows the sample tube holder next to a column carrier. This column carrier holds the columns and moves from the column-preparation area to the two sets of tube racks used for collecting the Glib and Hb (non-Glib) fractions. The column carrier, which serves as the rack for the chromatographic columns, imparts a fourth degree of freedom to the robot. Stations for microtiter plates are positioned for the performance of
‘Department of Pathology, University of Virginia Health Science Center, Charlottesville, VA 22908. 2Hanulton Co., Reno, NV 89520.0012. 3VA Medical Center Laboratory Service, 3350 La Jolla Village Dr., San Diego, CA 92161, and Department of Pathology, University of California-San Diego, La Jolla, CA 92122. 4Address correspondence to this author, at the VA Medical Center. Received January 6, 1992; accepted August 27, 1992.
Fig. 1. Layout of the Hamilton Microlab 2200 pipetting station Movable column-carrier racks enable the Instrument to move the columns to predeterminedpositions during the course of the assay
AddftlonalKeyphrases:chromatography, affinity
nomics
of
laboratory operation
Assays of glycohemoglobin (Glib) are widely used to the time-averaged blood glucose concentration over the preceding 6-8 weeks in diabetic patients. The methods used to quantify GHb include ion-exchange assess
chromatography (1), boronate affinity chromatography (2), and electrophoresis (3). Boronate affinity chroma-
tography
is an attractive
method for quantifying Glib, found in other quantification methods (4). Moreover, the method is not affected by slight changes in temperature, buffer ionic strength, labile GHb, or hemoglobin (Hb) variants (4). However, the procedures for quantifying Glib with boronate minicolumns are tedious and labor intensive. Two analytical approaches are available to resolve this problem. The first, high-performance liquid chromatography (HPLC), has recently been automated and uses bonded phenylboronic acid to bind the Glib. Alterna-
CLINICAL CHEMISTRY, Vol.
39, No. 1, 1993
143
the hemolysis step and to receive the aliquots of the Hb and Glib fractions for absorbance readings. We also used an Accuflex programmable pipetting device (ICN, Horsham, PA), which is equipped with a pipette oriented vertically over a platform that can travel in an x-y plane. The pipette is designed to move up and down (z direction). This semiautomated system requires prior hemolysis of the sample before analysis; it also requires that racks of tubes be changed midway through the analysis. The robotic pipetting stations have several common features. For example, in both, the liquid-air interface in the sample or reagent containers is detected by liquid-level-sensing hardware. All liquid-delivery steps are performed without the need to change the fluiddelivery syringes. (The Microlab 2200 is equipped with 5-mL and 500-jL syringes, the Accuflex with 10-mL and 200-zL syringes.) Both robotic pipetting stations are equipped with custom-designed hardware to perform the column chromatography. Software
We wrote custom-designed software for the Hamilton Microlab 2200, using FLEXPREP, a Basic-like software with pipetting commands; for the Accuflex, we wrote in Accuilex Basic. We used IBM-compatible computers that were attached to the pipetting stations through serial RS-232 connections. All pipetting station timing, movements, and buffer volumes pipetted were under software control.
2. Retrieve 50 L of washed, hemolyzed erythrocytes from each sample on the specimen rack and place this directly onto the column fit above the affinity gel. 3. Add 100 pL of First Fraction Elution Agent (see ref. 5) to the top of the column; allow the effluent to drain into the waste reservoir. 4. Move the rack over the first elution tube. Let the hemolysate sit on the resin on the top of the column for 10 mm before the next step. 5. Add 3 mL of First Fraction Elution Buffer to the column and collect the non-Glib eluate in 12 x 75 mm test tubes. 6. Add 17 mL of distilled water to each test tube. 7. Alert the technologist to remove the rack of patients’ samples and replace it with a second rack of empty tubes. 8. Add 2 mL of Second Fraction Elution Buffer to the column and collect the Glib eluate in 12 x 75 mm test tubes. At this point the test tubes containing the Glib and non-Glib fractions are removed by a technologist, thoroughly mixed, and placed manually in a spectrophotometer equipped to calculate the GHb%. We used a spectrophotometer from Source Scientific Systems Inc. (Garden Grove, CA). 9. Calculate GHb% from the absorbance values, alter blank correction, using the following formula: GHb%
=
100 x GHb/(GHb
(1)
+ lOHb)
where Glib = absorbance of the Glib fraction, absorbance of the non-Glib fraction.
and Hb
=
Chromatographic Columns
We used disposable Glyc-Affin Glib chromatography columns (Isolab, Akron, OH) for assays on both robotic pipetting stations. The 6.5-mL columns contained 0.25 mL of boronate affinity matrix consisting of Sepharosebound phenylboromc acid. This resin selectively binds the cis-diol functional group of the glucose that is bound to form the Glib. The automated robotic methods for Glib were adapted from the manual method used in our laboratory (5). Before each analysis, we filled the reagent bottles with buffer solutions, placed empty test tubes into racks on the beds of the Accuflex and Hamilton pipetting stations, and placed microtiter plates on the Hamilton. Affinity columns, which had been prepared according to the manufacturer’s instructions, were loaded into the column carriers. Accuflex
The Accuflex is equipped to perform GHb analysis on as many as 48 patients’ samples plus two control samples in each run sequence. After the robot checks by liquid-level sensing that all reagent containers are full, the run is initiated on the Accuflex by adding hemolyzed patients’ erythrocyte specimens to 12 x 75 mm test tubes. We programmed the pipette for the following sequence. 1. Wash the columns with 2 mL of column-preparation solutions and let this drain into the waste reservoir. 144
CLINICALCHEMISTRY,Vol.39, No. 1, 1993
Hamilton Microlab 2200 Briefly, the procedure for the Microlab 2200 was a modified, more completely automated version of the Accuflex procedure. All steps were similar except that the Microlab 2200 automatically performed the hemolysis procedure in a microtiter plate. Furthermore, the Hamilton procedure did not require a rack change or manual mixing of the elution fractions. On-board hemoiysis. Each patient’s sample (whole blood with EDTA anticoagulant) was placed in a labeled rack. The instrument was primed and fresh microtiter plates were placed in position. The pipette mixed each blood sample by initially aspirating 1000 L of the sample, then jet-dispensing 750 ML into the sample tube, followed by twice aspirating and jet-dispensing 750 MLof the sample. This completely mixed the blood sample. The initial aspiration removed an additional 250 ML of plasma from the top to the specimen, which would have been depleted of erythrocytes because of settling. This step increased the hematocrit of the remaining sample, thus allowing for greater absorbance readings during the quantification. After the miring was completed, the pipette was returned to the wash station, where the 250 ML taken from the top of the sample tube was flushed out. The pipette was then washed with 5000 ML of water. After the sample had been mixed and the pipette washed, the pipette moved to a beaker holding the
aspirated 200 ML of reagent, then moved to the sample tubes and aspirated 48 ML of a mixed whole-blood sample. The pipette dispensed the total 248 ML into the appropriate microtiter well. For proper mixing and complete hemolysis, 100 MLof the mix was twice aspirated and dispensed, all within the microtiter well. This was repeated for each sample. The control samples were manually pipetted into the appropriate wells of the microtiter plate. The Hamilton next performed steps 1-5, identical to those in the Accuflex sequence except that the hemolysate was obtained from a microtiter well and the nonGlib eluate collected in a 12 x 55mm test tube. The rest of the programmed sequence was as follows: 6. The robot moved the column carrier over the next set of collection tubes and added 2 mL of Second Fraction Elution Buffer to the column. The Glib eluate was collected in 12 x 55 mm test tubes. 7. While the Glib was being collected, the pipette was mixing each of the non-Glib fractions, just collected, by aspirating and jet-dispensing 750 ML of eluate, twice. The pipette then transferred 160 MLof non-GHb eluate from the test tube to the analytical microtiter plate. 8. The Glib eluate was also mixed by aspirating and jet-dispensing 750 MLof the sample fraction twice. The pipette then transferred 320 MLof the Glib eluate to the analytical microtiter plate. We then measured the absorbance of the microtiter plate wells by using a Bio-Tek (Winooski, VT) EL312 microtiter plate reader and calculated the GHb% from the absorbance values, after blank correction by using the following formula (terms as defined for equation 1): sample-peparation
reagent
GHb%
=
and
100 x GHb/(GHb
+
3Hb)
20) containing GHb ver the range of 2-20% were analyzed with the Microlab 2200 with both on-board and off-board hemolysis to determine whether this would affect results. Time study. This study was divided into two components: the hands-on time required of the technologist and the time per sample required for the instruments to assay the samples. The study was based on running 96 specimens (including controls). Each method was timed in two separate runs, with no noticeable between-run difference for any of the methods. Statistical methods. Data were subjected to linearregression analysis. Precision was evaluated by using the method described in NCCLS EP5 (6) for the alternative that included only one run per day. Comparison
of lysing
methods.
Specimens
(n
=
BloodSpecimens Whole blood collected into EDTA-cont.aining Vacutamer Tubes (Becton Dickinson, Rutherford, NJ) from discarded patients’ samples was used in this study. The specimens used in precision and linearity studies were stored at 4#{176}C until preparation of the hemolysates. Hemolysates were prepared from the erythrocytes within 24 h of collection and were stored at -70 #{176}C if not analyzed immediately. For patient comparison studies, the Hamilton sampled directly out of the Vacutainer Tubes.
Samples for the linearity study were prepared by mixing various proportions of a specimen containing 21.8% Glib with a specimen containing 6.6% Glib. We determined by absorbance measurements that the contrived specimens contained equivalent amounts of total hemoglobin (Glib + Hb).
(2) Results
Other Procedures CLC 330. The Primus CLC 330 (Primus Corp., Kansas City, MO) determines Glib by an HPLC-boronate affinity method. The high-performance liquid chromatograph is equipped with a 99-sample autosampler, a spectrophotometric detector (413 ± 2 nm), and a computing integrator. The 0.5 x 5 cm glass analytical column contains aminophenylboronic acid bonded to a 10-jm-thick rigid porous polymer support. The analytical sequence is as follows: Blood samples Primus
are manually hemolyzed by dilution of 10 .LL of whole blood with 990 12L of Glib diluentihemolysis reagent (Primus). Lysates are manually placed in vials and loaded into the autosampler. The samples are automatically injected onto the column. Glib binds to the column while lib is eluted with Elution Reagent 1 through the column to the spectrophotometric detector. Next, Elution Reagent 2 elutes Glib from the column to the detector. Column Regeneration Reagent is then added to prepare for the next sample sequence. The computing integrator calculates the Glib% by the following formula: GHb%
=
100 x Glib peak areal(GHb peak area + Hb peak area)
(3)
Linearity. The values obtained by multiple analysis (n =4) of the contrived samples containing a range of Glib values (6.6-21.8%) gave the following least-squares re-
gression equations: 4ccuflex, measured GHb% = 0.99(±0.02) calculated 0.31(±0.32) (SEE = 0.52, r = 0.993, n = 8); Hamilton, measured GHb% = (0.99 ± 0.01) calculated + (0.27 ± 0.19) (SEE = 0.31, r = 0.997, n = 8); Primus, measured GHb% = (1.01 ± 0.004) calculated + (0.25 ± 0.05) (SEE = 0.09, r = 0.999, n = 8). Precision studies. Results of the precision study for the Accuflex, Microlab 2200, and the Primus 330 are shown in Table 1. With the Accuflex, within-run standard deviations are very close to the total standard -
deviation,
whereas
for the Hamilton
they are about
half
of the total standard deviation. The Primus has remarkably small within-run standard deviations, with only a slight increase in the total standard deviation. Comparison of lysing methods. The comparison of %GHb results for 20 samples hemolyzed by on-board (y) and off-board (x) methods on the Hamilton analyzer gave the following least-squares regression equation: y = 0.98x + 0.2% (r = 0.997, S = 0.26, n = 20). Comparison of analytical methods. Blood specimens analyzed by both the Accuflex (x) and the Hamilton (y) gave the following least-squares regression equation: y CLINICAL CHEMISTRY, Vol. 39, No. 1, 1993
145
Table 1. PrecisIon of the Automated Methods for GHb GHb %
_________________ Normal
L-1
L-2
Mean
5.17
Swv
0.13 0.18
9.77 0.18 0.30
11.3 0.19
L-3
Hamilton (n = 25)
ST
15.0 0.21 0.41
0.44
Accuflex (n = 25) 5.40 0.29 0.29
9.70
4.77
10.1 0.09 0.10
11.4
0.44
0.40
0.47
0.53
15.0 0.52 0.54
Primus (n = 20)
Mean
0.07 0.08
11.4
15.2
0.09
0.09
0.11
0.12
8,,,, within-run standard deviation; S,., total standard deviation.
0.4% (r = 0.99, S = 0.40, n = 145). Samples by both the Hamilton (y’) and the Primus (x’) gave the following least-squares regression equation: y’ = 1.OOx’ 0.1% (r = 0.98, S = 0.38, n = 43). Time study. As Table 2 clearly shows, using any of the three robotic systems can save technologist time and +
-
also increase analytical throughput. to operate the Accuflex
required additional
time for specimen
The extra handling is reflected in the
throughput.
Although
the
Primus requires significantly less hand-on time, the longer analysis time is due to sequential analysis of specimens rather than parallel analysis. The more complete automation and parallel analysis of the Hamilton reduces the hands-on time and the total analysis time.
DIscussIon Many
analytical
in the clinical
techniques
laboratory
have been automated through the use of commercially available analyzers. Clinical analyzers achieve automated sample analysis through the use of hard automation, i.e., samplers, pipetter/diluters, photometers, and microprocessors. However, the main drawback of modera clinical automation is the lack of hardware flexibility and programmability. Considerable labor savings are possible through combining several laboratory operations into a single flexible laboratory robot (7). A system that can be programmed to meet initial laboratory needs and then reprogrammed as laboratory needs change will provide substantial equipment savings. The Microlab 2200 provides flexibility by allowing changeover to any of 26 immunoassays in