Serial estimation of motor unit numbers using an implantable system following nerve injury and repair in rats Michael P. Willand, Member, IEEE, and Joseph Catapano Abstract— Motor unit number estimation (MUNE) is an established technique to assess recovery following peripheral nerve injury. In rats, where the vast majority of peripheral nerve research is conducted, assessing motor units at various time points requires a terminal procedure due to the invasive nature of current techniques. Here, we present an implanted system that was used to serially assess MUNE after peripheral nerve injury and repair in rats. This system significantly increases the efficiency of peripheral nerve research by negating the need for terminal procedures, allowing for serial MUNE assessment over time in the same rat. Our system utilizes a commercial implantable stimulator, custom designed cuff electrode, and corresponding custom software with automatic M-wave classification to quickly assess functional reinnervation up to 8 weeks following nerve injury and repair. The concepts presented in this paper are applicable to any implanted device with a transcutaneous radio frequency or inductive link that can be used to trigger nerve stimulation. The methodology is also applicable to researchers without access to implantable devices.
I. INTRODUCTION Traumatic peripheral nerve injuries result in devastating functional deficits [1]. Optimal recovery occurs when the injured nerve is repaired immediately using a direct coaptation [2]. Recovery can be measured clinically using functional outcome measures [3], [4], however, several studies also use more objective measures such as motor unit number estimation (MUNE) techniques [5], [6]. In comparison to cruder functional outcome measures, MUNE estimates the number of axons, or motor neurons, that have regenerated to form functional connections within the muscle, providing a surrogate measure of nerve regeneration. Historically, the first method of MUNE involved gradually increasing the amplitude of an electrical stimulus delivered to the nerve while recording the corresponding compound motor action potential (CMAP) off of the surface of the skin. This technique, known as the incremental stimulation method, was first derived by McComas [7]. Each incremental increase to the stimulus amplitude results in the recruitment of an additional motor unit and produces a corresponding increase in the CMAP. To estimate the number of motor units in a muscle, a sample of motor unit responses are averaged to produce the average single motor unit potential (SMUP). The maximum CMAP is then divided by the SMUP to produce the MUNE. Other methods of MUNE stimulate the nerve at multiple points using low stimulation amplitudes obtaining *This work was supported by MED-EL GmbH, Innsbruck, Austria M.P. Willand (
[email protected]) and J. Catapano are with the Division of Plastic Reconstructive Surgery at the Hospital for Sick Children, Toronto, ON M5G 1X8, CANADA.
978-1-4577-0220-4/16/$31.00 ©2016 IEEE
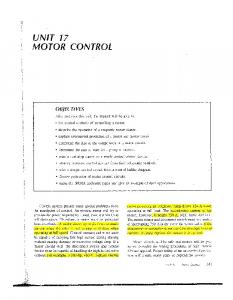
just a single motor unit potential and averaging the result [8]. MUNE is then calculated in a similar manner by dividing the CMAP by the average SMUP. MUNE has also been used to provide assessments of functional neuromuscular connections in animal models of spinal cord injury [9], neuropathies, such as amyotrophic lateral sclerosis [10], neurodegenerative disorders, such as Parkinsons disease [11], and peripheral nerve injury [12]– [14]. In the majority of studies, animals must be sacrificed following MUNE procedures as it requires the surgical exposure of either the muscle and corresponding nerve or the severing of a muscular tendon for connection to a force transducer. This prevents researchers from assessing the same animal serially over time, limiting their ability to investigate how MUNE recovers over time without significantly increasing the number of experimental animals. While some studies have been able to demonstrate serial MUNE assessments in the same animal using needle stimulation and recording techniques [15], these methods are dependent on the experience of the experimenter and may produce different results depending on the placement of the recording electrodes. In this paper we present a system based on interfacing a commercial implantable stimulator for providing direct nerve stimulation with an implanted cuff electrode and implanted electromyogram (EMG) recording electrodes. We tested this system over an 8-week period in rats following peripheral nerve injury and repair. II. METHODS A. System Design A block diagram of the overall setup is shown in Fig. 1. Custom designed software written in LabVIEW was interfaced to a data acquisition device and used to trigger an implantable stimulator through an inductive link and synchronize recording of EMG potentials. EMG signals were amplified using an A-M Systems Model 1800 amplifier. The implantable stimulator was provided courtesy of MEDEL GmbH and was interfaced to a three contact cuff electrode. Contact spacing was 0.5 mm and cuff diameter was 1 mm. Having three contacts for stimulation allowed us to perform the incremental MUNE procedure at two different stimulation sites (with a bipolar electrode arrangement using two of the cuffs contacts) and then average the two results. This method is a hybrid multiple point stimulation/incremental MUNE technique. Two stainless steel wires (Cooner Wire, AS 631) served as EMG recording electrodes and were implanted intramuscularly.
323
刀愀琀
䰀愀戀嘀䤀 䔀圀 倀爀 漀最爀 愀洀 一愀琀 椀 漀渀愀氀 䤀 渀猀 琀 爀 甀洀攀 渀琀 猀 䐀䄀儀
䤀 渀搀甀挀 琀 椀 瘀攀 䰀椀 渀欀
䔀䴀䜀 䄀洀瀀氀 椀 昀 椀 攀 爀
䤀 洀瀀氀 愀渀琀 愀戀氀 攀 匀琀 椀 洀甀氀 愀琀 漀爀
䔀䴀䜀 䔀氀 攀 挀 琀 爀 漀搀攀 猀
Fig. 1. Block diagram of implantable motor unit number estimation setup.
B. Classification of Recorded Motor Unit Potentials The LabVIEW software provided a graphical user interface (Fig. 2) to allow visualization of the recorded motor unit potentials. It also served to allow manual control of stimulation amplitudes. This is important as it allows familiarity with performing the MUNE procedure for those that have performed the procedure in the past using isolated stimulus units where manual control of the amplitude is essential (i.e. Grass SD9, Digitimer DS7A, or equivalent). Automatic classification of recorded EMGs was performed using a Wavelet pattern recognition scheme [16]. Briefly, each recorded signal was bandpass filtered from 10-500 Hz and then a 3-level wavelet decomposition using the Daubechies 4 wavelet was performed in real-time. The sum of the Euclidean distances between the third level wavelet approximation coefficients of the current EMG response was compared to a discriminator value and then the current response was either classified as a new template or allocated to an existing template. This classifier and associated software has previously been used to determine motor unit numbers in various rat and human studies [12], [13], [16]. In all cases, data was similar to published results by others which validated the methodology used.
is important when implanting devices into rats. All surgical procedures and assessments were approved by The Hospital for Sick Children Laboratory Animal Services (LAS) and performed according to the Canadian Council on Animal Care Guidelines. Rats were anesthetized with 2% isofluorane and, using aseptic technique, two incisions were made (Fig. 3). Through the mid-thigh incision, a subcutaneous pocket was created in order to place and anchor the implantable stimulator on the back. Also through the mid-thigh incision, the tibial nerve was exposed and transected approximately 12 mm from the entry into the gastrocnemius muscle and immediately repaired using two 9-0 nylon sutures. The cuff electrode that was connected to the implantable stimulator was then implanted proximal to the site of nerve repair and was kept in place with a 6-0 polypropylene suture to ensure the cuff did not migrate. A second incision on the dorsal aspect of the lower limb was used to expose the gastrocnemius muscle. Two Teflon coated stainless steel wires (Cooner Wire, AS 631) with tips bared of insulation were implanted into the muscle and anchored using 5-0 prolene suture. The distance between the electrodes was approximately 1 cm. These electrodes were used to record EMG and were threaded subcutaneously and exposed at the neck to connect to an external amplifier.
Fig. 3. Surgical implantation setup in a rat showing the two incision sites and implanted stimulator. Incision site #1 was used to access the tibial nerve and also to implant the cuff electrode and implantable stimulator. Incision #2 was used to access the gastrocnemius muscle for implantation of EMG electrodes.
Fig. 2. Front panel view of the graphical user interface that controls the implantable stimulator and also allows for visualization of characterized motor unit recordings. The raw input is shown in the top middle graph. On the right side are graphs of individual characterized templates. The large graph in the middle left plots all characterized templates in one graph.
C. Animals and Surgical Procedures We tested our system in four female Sprague Dawley rats weighing approximately 300 g. We chose to use females as their size and weight are maintained over time, which
Rats were assessed weekly for 8 weeks starting one-week post nerve injury and repair. In order to accurately perform the MUNE procedure rats needed to be anesthetized. Without anesthesia, voluntary EMG potentials may contaminate the evoked potentials leading to incorrect assessments of the number of functional connections within a muscle. The MUNE procedure first obtained the maximum compound motor action potential (CMAP) and then proceeded to incrementally increase stimulus amplitudes starting from zero. Once a maximum of 20 unique templates were found the procedure was stopped. In cases where 20 templates were not able to be obtained the procedure was stopped after 3 minutes. This situation arose during the early reinnervation phase 2-3 weeks post nerve injury and repair.
324
Our system performed as designed over the 8-week implantation period. Despite the large size of the implanted stimulators, all rats were able to move freely within their cages. At one-week post nerve injury and repair we were not able to elicit any muscular responses which is in line with previous reports. Values for maximum compound motor action potentials slowly increased over time (Fig. 4). As more axons reconnected with the denervated muscle fibers, stimulation of the proximal nerve stump enabled greater contraction of the muscle, which was evident from the CMAP results.
trodes were explanted. We observed a normal amount of scar tissue and encapsulation around both the stimulator and cuff electrodes. Once dissected free of the encapsulating tissue the cuff electrode was examined and showed no signs of damage or oxidation. The underlying nerve also appeared normal, providing confirmation that the implanted cuff electrode and serial MUNE procedure did not damage the repaired tibial nerve. 2 1
Amplitude (mV)
III. RESULTS
Maximum CMAP ( mV)
25 20
-1 -2
15
-3
10
-4
0
1
2
3
4
5
6
7
8
Time (ms)
5 0
Fig. 6. EMG responses from one rat taken at 4 weeks post nerve injury and repair. These responses were classified as unique templates by our LabVIEW software. The maximum compound action potential is not shown.
0
2
4
6
8
Time (weeks)
IV. DISCUSSION
Fig. 4. Peak to peak responses of the maximum compound motor action potentials (CMAP) measured from the gastrocnemius muscle (n = 4) recorded at 1 week intervals following tibial nerve injury and repair. There were no observable responses at one-week post nerve injury and repair. Error bars represent standard error of the mean.
These values also correlate to the number of estimated motor units shown in Fig. 5. We were able to serially observe muscle reinnervation in each rat. The intramuscular electrodes implanted into the gastrocnemius were able to record robust EMG responses. A sample of recorded muscle action potentials taken from one rat at 4 weeks post nerve injury and repair is shown in Fig. 6. 150
# Motor units
0
100
50
0
0
2
4
6
8
Time (weeks) Fig. 5. Gastrocnemius muscle motor unit number estimates (n = 4) performed weekly following tibial nerve injury and repair. There were no observable responses at one-week post nerve injury and repair. Error bars represent standard error of the mean.
Eight weeks following nerve injury and repair rats were sacrificed and stimulator units with corresponding cuff elec-
The results shown here validate our system for serially measuring reinnervation in rats. The implanted stimulators were tolerated well in all experimental animals and serial evaluation resulted in no apparent nerve damage or inhibition of reinnervation. Interestingly, in comparison to previous results in our own lab, we found that serially performing MUNE in the same rat actually increased reinnervation of the muscle [13]. This previous work was performed using an identical nerve injury and repair model as the one outlined in this paper, with the only difference in experimental design being that MUNE was only assessed at terminal endpoints and not serially. Therefore, no stimulation was performed after the nerve repair in those rats. At 4 weeks after nerve injury and immediate repair, we found 38 ± 8 motor units in gastrocnemius muscles that were serially assessed, a significantly greater number than the 22 ± 2 motor units found previously when MUNE was assessed only with a terminal procedure (p