Radiology
James E. Stahl, MD, CM, MPH Karen L. Furie, MD Suzanne Gleason, PhD G. Scott Gazelle, MD, MPH, PhD
Index terms: Brain, infarction, 13.78 Cost-effectiveness Economics, medical Radiology and radiologists, socioeconomic issues Tissue plasminogen activator (TPA) Published online 10.1148/radiol.2283021557 Radiology 2003; 228:659 – 668 Abbreviations: NINDS ⫽ National Institute of Neurological Disorders and Stroke QALY ⫽ quality-adjusted life year tPA ⫽ tissue plasminogen activator 1
From the Institute for Technology Assessment (J.E.S.) and Departments of Radiology (J.E.S., G.S.G.), Medicine (J.E.S.), and Neurology (K.L.F.), Massachusetts General Hospital, Harvard Medical School, Zero Emerson Bldg, Suite 2H, Boston, MA 02114; and Department of Economics, Trinity College, Hartford, Conn (S.G.). Received November 25, 2002; revision requested February 4, 2003; revision received March 31; accepted April 10. Supported in part by the U.S. Department of the Army with DAMD 17-992-9001. Address correspondence to J.E.S. (e-mail:
[email protected]).
The information does not necessarily represent the position of the government, and no official endorsement should be inferred.
Author contributions: Guarantor of integrity of entire study, J.E.S.; study concepts, all authors; study design, J.E.S., G.S.G.; literature research, J.E.S., S.G.; data acquisition, J.E.S., S.G., K.L.F.; data analysis/interpretation, all authors; statistical analysis, all authors; manuscript preparation, definition of intellectual content, editing, revision/review, and final version approval, all authors
Stroke: Effect of Implementing an Evaluation and Treatment Protocol Compliant with NINDS Recommendations1 PURPOSE: To evaluate—relative to routine clinical practice—the potential costeffectiveness of implementing a strategy compliant with National Institute of Neurological Disorders and Stroke (NINDS) recommendations for care of patients presenting with signs and symptoms of acute ischemic stroke. MATERIALS AND METHODS: A discrete-event simulation model of the process of stroke care from symptom onset through administration of tissue plasminogen activator (tPA) was constructed. A literature review was performed to determine process times, performance of computed tomography (CT), health outcomes, and cost estimates. The following were compared: (a) a “base-case” strategy determined on the basis of findings in the literature and (b) a NINDS-compliant strategy (ie, evaluation by emergency physician in less than 10 minutes, interpretation of CT scans within 45 minutes, and administration of tPA within 1 hour after presentation). Strategies were compared with regard to cost and effectiveness. Sensitivity analyses were performed for all relevant cost, timing, and resource parameters. Outcomes of concern were quality-adjusted life years and number of patients treated within a 3-hour therapeutic window. RESULTS: The NINDS-compliant strategy resulted in an average quality-adjusted life years value of 3.64, versus 3.63 for the base case, at an approximate cost of $434 per patient. The NINDS-compliant strategy increased the proportion of treatable patients from 1.4% to 3.7% and remained cost-effective for expenditures of up to $450 per patient. Assuming base-case parameters are used, increasing the number of CT scanners from two to eight raised the proportion of treatable patients to 1.5%. Increasing the number of available neurologists from four to eight raised the proportion to 1.44%. Reducing the time from stroke onset to emergency department arrival by 30 minutes raised the proportion to up to 7.7%. CONCLUSION: Applying NINDS recommendations is potentially cost-effective, although reducing the time from stroke onset to emergency department arrival may be even more so.
More than 3 million cases of stroke are reported every year (1), and approximately 83% of these strokes are ischemic (2). Although not all individuals seek emergent care, more than 498,000 patients with ischemic stroke—20% of whom had recurrent stroke—were seen in U.S. emergency departments (3) in 1999 alone. Stroke is the third leading cause of death in the United States and is a source of disability for more than 4.5 million survivors. Estimates of the cost of caring for patients with stroke range from $20 billion to more than $40 billion each year (4). In 1995, the average cost of a stroke-related hospitalization alone was estimated to range from approximately $12,000 (5) per patient discharged from the hospital to more than $20,000 (6) for patients with the most severe ischemic strokes (ie, 4 or 5 on the modified Rankin Disability Scale [7]). Intravenous tissue plasminogen activator (tPA) is currently the only agent approved by 659
Radiology
TABLE 1 Timing Data
Interval between Events
Median (h)
Mean (h)
Range (h)
No. of Patients
Reference No.
From stroke onset to calling emergency medical services* From stroke onset to emergency department† From emergency department arrival to evaluation by emergency physician From emergency department arrival to neurologic evaluation From emergency department arrival to CT scanning From emergency department arrival to administration of thrombolytics (typically tPA)
2.42 1.53
2.68 3.11
0.5–6.0 0.96–18.81
353, 682 3,742
8, 17–20 17–19, 21–27
0.33
0.41
0.3–0.6
2.75 1.63
3.32 1.67
2.42–4.19 0.5–6.78
1,508 1,879
NC
1.62
1.03–2.20
37
928
NINDS Recommendation (h)
22, 26
0.167
27, 28 18, 22, 26–29
0.25 0.41
29
0.75
Note.—All estimates are weighted by the combined number of patients in the studies. CT ⫽ computed tomographic, NC ⫽ not calculated, NINDS ⫽ National Institute of Neurological Disorders and Stroke. * Not all researchers reported mean and median values for the interval between onset of stroke symptoms and calling emergency medical services. Median values were reported for a total of 353 patients, and mean values were reported for a total of 682 patients. † For patients arriving less than 24 hours after stroke onset (approximately 14% of patients in these studies arrived more than 24 hours after the onset of stroke symptoms).
the U.S. Food and Drug Administration for treating acute ischemic stroke. Results of several large studies (8 –12) have shown that intravenous tPA, if administered within 3 hours after an acute ischemic stroke, may result in improved function—as measured with several validated stroke outcome scales (7,13–15)— at both 90 days and 1 year after stroke. Although there is some evidence that in selected patients (ie, those with middle cerebral artery embolic occlusion) this window of therapeutic opportunity may be as long as 6 hours with catheter-directed thrombolytic treatment (16), data with regard to long-term morbidity and mortality in these patients are very limited. In addition, these patients may also represent a very different population from those presenting to the hospital within 3 hours. A major problem in treating patients with acute ischemic stroke is that few arrive and/or are evaluated and treated within the 3-hour therapeutic window. A systematic review of the literature performed by J.E.S. revealed the timing of events in current practice from stroke onset through evaluation and management (Table 1). The average time for in-hospital evaluation to treatment is more than 1.5 hours. This means that, on average, a patient in the community experiencing an ischemic stroke must be recognized and delivered to the hospital in less than 1.5 hours to receive tPA in time. Depending on the study (8,10,11,16,21,30), only 0% and 3% of patients with ischemic stroke were found to do so. This is a consequence of delayed recognition of stroke in the community, delays in traveling to the emergency department (17,18,21–26,28,31), 660
䡠
Radiology
䡠
September 2003
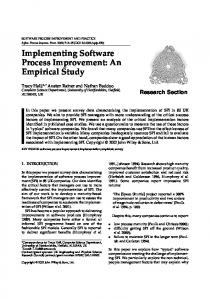
and variability in the care provided to patients with stroke when they arrive at the hospital. To help manage intrahospital care, the NINDS has published recommendations as to how long the process between evaluation and treatment should take once the patient arrives at the hospital. NINDS recommendations (32) are that from the moment of arrival at the emergency department, a patient with stroke symptoms should be evaluated by an emergency medicine physician within 10 minutes, a neurologist should be contacted within 15 minutes, CT of the head should be performed within 25 minutes and CT findings should be interpreted within 45 minutes, tPA should be administered within 1 hour, and the patient should be admitted to a supervised room within 3 hours (Fig 1). The main purpose of our study was to evaluate the potential cost-effectiveness—relative to routine clinical practice— of implementing a strategy for the care of patients with acute ischemic stroke that is compliant with NINDS recommendations.
NINDS strategy. This is the relative difference in the cost of providing care with the NINDS-compliant strategy divided by the change in health outcome as compared with current practice. The health outcome measure used was quality-adjusted life years (QALYs) (33). In our analysis, the costs and benefits of the stroke evaluation and management system were calculated for the entire presenting population, not just those who are preselected to benefit from tPA. The analysis was performed in this way because the stroke evaluation and management system operates in the context of the general population, not in a preselected group; it involves attempting to evaluate and manage all patients presenting with stroke symptoms regardless of whether or not they are actually having a stroke. This analysis was performed from the societal perspective. A computer simulation model capturing the costs, health outcomes, timing, competition for resources, and resource utilization aspects of the process of care was used to compare these two strategies.
Model MATERIALS AND METHODS We performed a cost-effectiveness analysis comparing an evaluation and treatment strategy that is compliant with NINDS regulations (this strategy is hereafter referred to as a NINDS-compliant strategy) with current practice. Both strategies are described in detail below in the Strategy Description section. The measure of benefit used was the incremental cost-effectiveness ratio for the
A discrete-event simulation modeling approach was chosen. The model was developed by using SIMAN (Rockwell Software, Sewickley, Pa), a general-purpose discrete-event simulation language, with the Arena software platform (Rockwell Software). Discrete-event simulation (34,35) is a computer modeling method in which entities (eg, patients) within a system may interact and/or compete with each other for resources, such as CT time. In Stahl et al
Radiology
Figure 1. Flowchart shows timing of events in current practice and in proposed NINDS recommendation– compliant strategy. ⴱ ⫽ start of in-hospital evaluation and management, ED ⫽ emergency department, EMS ⫽ emergency medical services, EP ⫽ emergency medicine physician.
addition, the system being evaluated may be modeled to allow discrete and abrupt changes at variable times rather than being constrained to have changes occur at fixed time intervals, as semiMarkov models are. For example, patients may “enter” the modeled system at any time, and the time needed for evaluation and care may vary from patient to patient. The probability of events, the duration of processes, and the rate at which people may enter the system are typically derived from random and independent sampling from theoretical or empirically derived distributions. This type of simulation is designed to capture flow time, waiting time, and competition for resources. It also permits the analyst to examine the interdependence of events, thereby providing insight into system dynamics and bottlenecks such as those that might occur in busy city hospitals.
Strategy Description Two treatment strategies were compared: current clinical practice and a NINDS-compliant strategy. Both strategies involved tracking stroke care through the following steps: 1, symptom onset; 2, arrival at emergency department; 3, thorough evaluation by an emergency medicine physician; 4, CT scanning and Volume 228
䡠
Number 3
interpretation of CT findings; and 5, administration of tPA to eligible patients. In the model (Fig 2), it is assumed that steps 1 through 5 are sequential. One exception is the role of the neurologist. Neurologists are contacted either before the patient’s arrival at the emergency department by emergency medical services personnel or at emergency department arrival by the emergency medicine physician. Once contacted, a neurologist must perform a clinical evaluation of the incoming patient and a radiologist must interpret the results of the head CT before the patient can receive tPA. Once this task has been completed, the neurologist is free to evaluate and treat the next patient. In this study, current practice was defined as the process of evaluating and caring for patients with stroke in tertiary care centers, with the times needed to complete the aforementioned steps derived from a systematic review of the published data (8 –12,17–31,36 – 44). These data are reported in the Reference Case Assumptions section. The NINDScompliant strategy incorporates the times recommended by NINDS (20,44). After their discharge from the hospital, patients reenter the community, where they may eithe eventually die a non– stroke-related death or experience a re-
current stroke, whereupon they reenter the evaluation and care process. In both strategies, patients with intracerebral hemorrhage, subarachnoid hemorrhage, or subdural hematoma were not considered for thrombolytic therapy. These patients were assumed to receive standard therapy for intracranial bleeding—specifically, intubation with hyperventilation, mannitol administration, and elevation of the head of the bed, followed possibly by intracranial pressure monitor placement and, potentially, surgery as early as 24 hours after presentation (45,46). The volume and location of the hematomas are the primary determinants of prognosis in these patients. Therefore, the NINDS protocol would not have a substantial effect on the care these patients received or on their outcome. It should also be noted that when one is comparing strategies, any intervention that is identical across strategies—and in this case the same proportion of patients with hemorrhagic stroke were assumed to present in each strategy—will not contribute to any potential marginal benefit. A literature review was performed to determine the best estimates for patient arrival rates, process times, CT examination characteristics, expected outcomes, in-hospital and outpatient costs for both treated and untreated patients, and quality of life. These values and their sources are reported in Tables 1–5. For the NINDS-compliant strategy, the time to emergency medicine physician evaluation was constrained to a uniform distribution between 5 and 10 minutes, and the time within which the neurologist would be contacted was set as a uniform distribution between 5 and 15 minutes from patient arrival. The time to CT scanning was constrained to a uniform distribution between 10 and 15 minutes after evaluation by the emergency medicine physician, the reading of CT results was set as a uniform distribution between 5 and 20 minutes after head CT, and tPA administration was constrained to a uniform distribution between 5 and 15 minutes after the reading of CT scans (Fig 1). The lower limits were based on the expert opinion of one of the coauthors (K.L.F.). A uniform distribution was assumed because in the protocol, it is only specified that the events occur within the specified time frame. Use of any other distribution would explicitly bias the assumption of how long these processes might take. Triangular and other distributions were used when more data were available about the behavior of the process. The effectiveness of therapy was based
Implementing a Stroke Protocol Compliant with NINDS Recommendations
䡠
661
Radiology
Flowchart shows stroke evaluation and management model. CAT Scan ⫽ CT scanning, N ⫽ no, Y ⫽ yes.
Figure 2.
on the results of the NINDS recombinant tPA trial (10). The outcome measures were survival rate and improvement in functional outcome as measured by modified Rankin score (a measure of global function) at 10, 90, and 180 days and at 1 year (10,55). In the model, each patient’s survival and health state were evaluated at these intervals after discharge from the hospital for a stroke. In the model, the surviving patients’ health state was allowed to worsen, improve, or remain the same at these times. This probability of changing from one health state to the next was based on changes in the distributions of the patients’ Rankin scores at the beginning and at the end of the evaluation intervals as reported in the NINDS recombinant tPA trial (10). A simplifying assumption in the model for this initial analysis was that annual poststroke mortality and stroke recurrence rates after 1 year were the same for all patients, regardless of the severity of the initial stroke (70). In addition, after 1 year, a patient’s Rankin score was assumed to remain constant unless he or she had sustained another stroke.
Health Outcomes The health outcome measure used in the model is the QALY, as defined by Gold et al (33) (ie, a year lived as weighted by the quality of life during that time). A patient’s quality of life depends on his or her current health state. Each modified Rankin score category was considered a health state. These were categorized as follows: A modified Rankin score of 0 indicated no symptoms; a Rankin score of 1, symptoms but no disability; a Rankin score of 2, slight disability; a Rankin score of 3, moderate disability; a Rankin score of 4, moderate to severe disability; and a Rankin score of 5, 662
䡠
Radiology
䡠
September 2003
TABLE 2 Epidemiology and Probability Data Probability
Mean
Stroke patients requiring CT per hour per 100,000 persons Nonstroke patients requiring CT per hour per 100,000 persons Age-adjusted stroke death rate per 100,000 persons Discharge to nursing home from rehabilitation facility Stroke type Ischemic Intracerebral hemorrhage Subarachnoid hemorrhage Stroke recurrence rate
0.03 0.5 25.1 0.18 0.83 0.10 0.07 0.052
Range
Reference No. 47
18.3–42.5 0.13–0.21
3 48 49–51 2
0.03–0.08
49–54
Note.—Where available, ranges are provided.
severe disability. The quality of life or utility for each health state was modeled in the manner of Fagan et al (55) (ie, by mapping patient preferences to the postadmission modified Rankin score) and based on the results of published patient preferences for stroke health outcomes (55– 62). These are represented on a 0-to-1 scale, with 0 representing death and 1 representing perfect health. These values were derived by using the time– trade-off method and/or a visual analog scale (55– 64). The utilities for these categories and ranges are listed in Table 4.
Costs All baseline costs were adjusted to year 2000 U.S. dollars and were based on either national or local estimates. These costs were broken down into cost per day of hospitalization (55), cost of tPA (65,71), cost for physician time, intensive care unit costs for patients receiving tPA (65,71), and costs for rehabilitation and nursing homes (68,70). The model-generated costs were verified by comparing the cost per patient and its variability to independent global estimates for stroke hospitalization costs
(65). Length of hospital stay, a major contributor to costs, was, on average, approximately 15% shorter for treated patients than for untreated patients (11,30,37,39). Posthospitalization costs depended on the patients’ outcome. Patients could either be discharged to home alone, into the care of an outpatient rehabilitation facility, or to a nursing home (12%–15%) (37). Patients with little or no disability (ie, with a Rankin score of 0 or 1) were assumed to undergo a brief period of outpatient rehabilitation and then be discharged to home. Patients with a Rankin score of 2 or higher were assumed to go to an inpatient rehabilitation facility and subsequently to be admitted to a nursing home. Rehabilitation costs were based on the findings of Lee et al (68). The cost of days of lost work was based on the average daily wages reported by the U.S. Bureau of Labor Statistics (72). The cost of days of lost work was then multiplied by the number of days spent in a hospital, rehabilitation facility, or nursing home. All costs and health outcomes were discounted at 3% per year according to the technique of Gold et al (33). Stahl et al
Radiology
TABLE 3 Percentages of Patients in Given Health States (Rankin Categories) at Given Times after Stroke 10 Days (%)
Rankin Category 0 1 2 3 4 5 Dead Total
3 Months (%)
6 Months (%)
1 Year (%)
No tPA
tPA Therapy
No tPA
tPA Therapy
No tPA
tPA Therapy
No tPA
tPA Therapy
7 10 9 9 28 25 10
16 17 8 9 22 20 7
11 16 12 14 20 7 21
18 24 7 13 14 6 17
11 18 11 17 14 6 24
19 22 8 14 10 5 21
11 17 12 13 12 6 30
20 22 8 13 6 5 26
100
100
100
100
100
100
100
100
Note.—Data are derived from reference 10. Percentages may not add up to 100% due to rounding.
TABLE 4 Patient Health State Preference Data Rankin Category
Mean
Range
0, no symptoms 1, no disability despite symptoms 2, slight disability 3, moderate disability 4, moderate to severe disability 5, severe disability Death
0.90 0.79 0.68 0.65 0.40 0.32 0.00
0.85–0.95 0.70–0.90 0.35–0.90 0.20–0.90 0.12–0.54 ⫺0.20–0.54* 0.00
Note.—Data are from references 55– 64 and are utility scores. Weighted means are provided where more than one reference was available and the utility elicitation method used was the same. Extreme values are derived from minimum and maximum values reported in the references. * The first value (⫺0.20) was reported in reference 36 and springs from the fact that the 117 respondents in this study ranked a Rankin score of 5 as a worse outcome than a fatal stroke. (This may have been due in part to framing considerations—a fatal stroke in this study was characterized as rendering the patient unconscious and without pain, with death occurring several hours later without the individual ever waking.)
Process Times Process times were derived from a systematic review of the literature. Weighted mean and median scores were determined in this review. Where the percentage of arrival within specific hourly intervals was reported with sufficient frequency (as for the interval between stroke onset and emergency department arrival), a weighted mean for each interval was determined, and a cumulative probability distribution was fit to the weighted means. Where only median values were reported, a triangular distribution was fit to the weighted median, and the highest and lowest interquartile range values were reported. NINDS process times were estimated (K.L.F., J.E.S.) as uniform distributions according to expert opinion. The estimates available from the literature are reported in Table 1. Patient interarrival time, the rate at which patients with and without stroke have events, and calls on the resources of the system were derived from the National Ambulatory Medical Care Survey (3) (Table 2). We tested the validity of the model by Volume 228
䡠
Number 3
comparing its output with the published data. For example, within the group of patients in each strategy in our model, those who arrive and are treated within the therapeutic window spend a mean of 12.6 days (range, 11.4 –14.0 days) in the hospital, versus 15.5 days (range, 9.6 – 21.0 days) for those who do not receive treatment. The proportion of patients with a Rankin score of 0 or 1 at 1 year after discharge is 42% for those who receive therapy and 28% for those who do not. These output data are consistent with those in published reports (8,10 – 12,30).
Reference Case Assumptions The reference case patient was a 65year-old man with an average mortality rate (73). The reference case timing parameters were as follows: mean time from stroke onset to calling emergency medical services, 2.4 hours; mean time from onset of stroke to arrival at the nearest emergency department, 3.1 hours; mean
time from emergency department arrival to evaluation by an emergency medicine physician, 0.41 hour (25 minutes); and mean time from emergency department arrival to treatment, 1.6 hours. Patients who did not arrive in time to receive tPA received supportive care. In the reference case analysis it was assumed that, per Tilley et al (39), compliance with NINDS recommendations does not incur any new direct costs. Intracerebral hemorrhage caused by tPA was assumed to occur 6% of the time in the base case and always resulted in death. The baseline incidence of stroke was based on the general population estimate of 1.3% per year and on the number of reported emergency department visits for stroke per year. Sensitivity analyses were performed up to rates of 11%— the stroke rate for all patients aged 65 years and older (according to data from the National Center for Health Statistics for 1994 [73] and data from the U.S. Census for 1990 [74]). Other nonstroke patients were assumed to compete for the CT resource as well. The base population size was assumed to be 300,000 (the median U.S. city size [74]), which implies that, on average, more than 12 nonstroke patients per day compete for the emergency department CT unit (3,4). In our institution, Massachusetts General Hospital, which is an urban teaching hospital with more than 500 beds in Boston, the CT volume is approximately 60 patients per day. Using our institution as a reference, we also assumed that there were two CT scanners available to the emergency physicians. We chose this volume as being more representative of the kind of institution where a NINDS protocol would probably be first applied. Each of these assumptions was examined through sensitivity analysis.
Implementing a Stroke Protocol Compliant with NINDS Recommendations
䡠
663
Radiology
Sensitivity Analysis Sensitivity analysis is a method for testing the validity of the conclusion of a decision analysis. Sensitivity analysis tests the stability of the conclusions of an analysis across a range of probability estimates, value judgments, and structural assumptions (75). The variables that are varied are those about which the least is known and/or those that are most important to the analysis. For example, the cost of becoming NINDS compliant or the sensitivity of CT for detecting a stroke may be varied in a sensitivity analysis. Systematically varying these variables allows the experimenter to determine which variables are most important in the decision-making process. If the outcome of interest varies greatly or if the relative strength of the alternative strategies changes with the varied input parameter, then one considers the model to be sensitive to that parameter. If the outcome of interest does not vary significantly with the variable, then the model is considered to be insensitive to that parameter. Finally, more than one variable may be varied at a time. This allows us to identify configurations in which systems perform optimally. The central questions of this study relate to the relationship between the process and cost of stroke evaluation and management and the resulting health outcomes. In our examination, we varied the cost per patient for administering a NINDS-compliant protocol, as well as the following key timing and resource parameters: time from stroke onset to emergency department arrival, time from emergency department arrival to CT scanning, CT interpretation time, and length of the therapeutic window. With regard to resource parameters, we varied the number of available neurologists and CT scanners. The volume of stroke and nonstroke patients who “compete” with each other for CT time was also examined. Because there are little data to guide estimation of the cost of becoming NINDS compliant, this was examined as a toll for every patient evaluated.
RESULTS Reference Case Results The NINDS-compliant strategy was both cost saving and more effective than routine care (see Table 6). The reference case cost-effectiveness analysis whose results are shown in Table 7 was performed from the societal perspective. In this analysis, we examined the process of de664
䡠
Radiology
䡠
September 2003
TABLE 5 Economic Data Parameter*
Mean
Mean cost per admission for ischemic stroke ($) Average wholesale price of tPA ($) Physician cost for administration of tPA for 2 hours ($) ICU cost for observing patients receiving tPA for 1 day ($) Non-ICU hospital cost per day ($) Length of stay in hospital (d) Treated with tPA Untreated Inpatient rehabilitation ($) Outpatient rehabilitation ($) Nursing home cost per year ($)
Reference No.
Range
11,122 2,750 157
10,365–11,880
65 66 67
2,616 613
1,746–3,487
56 56 11, 30, 37, 39
13.5 16 23,898 2,517 49,190
9.7–17 9.5–21 11,255–45,020 1,351–2,814 24,597–61,494
50 68 69
Note.—Weighted means are provided where more than one reference was available. Ranges are given where available. All dollar costs reported in the references have been inflated to year 2000 U.S. dollar costs. * ICU ⫽ intensive care unit.
TABLE 6 Base Case Analysis Outcomes Health outcomes Life expectancy Quality-adjusted life expectancy Percentage of presenting patients receiving treatment within therapeutic window Economic outcomes Hospitalization cost Nursing home cost Outpatient costs including rehabilitation Total cost
Average with Current Practice
Average with NINDS Recommendations
Average Difference
9.58†
9.59†
0.009†
NS
3.63†
3.64†
0.01†
NS
1.4
3.7
2.3
P Value*
⬍.001
22,982‡ 35,563‡
22,924‡ 35,578‡
58‡ 15‡
NS NS
11,465‡ 69,539‡
11,296‡ 69,105‡
169‡ 434‡
NS NS
* NS ⫽ nonsignificant. † Data are years. ‡ Data are dollars.
livery of care and not the specific treatment. This means that all costs and effects in each strategy were averaged across all persons presenting with stroke symptoms, whether they were treated or not treated with tPA. Given the base case assumptions, the NINDS-compliant strategy resulted in an average QALY value of 3.64 (as compared with 3.63 with the current practice strategy) at an average cost saving of approximately $434 per patient (Table 6). Here, the costs and benefits of the strategies were spread across all presenting patients. Individually, the QALY value for a patient not treated in time was 3.62, versus 3.99 for a patient who did receive treatment in time. The cost savings came primarily from reduced hospital costs and reduced rehabilitation and nursing home costs.
In the reference case, approximately 40% of patients arrived within 3 hours of stroke onset. However, approximately 70% of these patients arrived at least 2 hours after stroke onset, leaving them with only 1 hour in which to receive treatment if deemed appropriate. Results of our base case analysis predict that 1.4% ⫾ 0.10 (SD) of patients would receive treatment if cared for according to current practice. Use of the NINDS-compliant strategy would increase this proportion to 3.7% ⫾ 0.19.
Results of Sensitivity Analyses Results of sensitivity analysis of cost per presenting patient revealed that a NINDS-compliant strategy was cost saving relative to current practice, although it was sensitive to the cost of implemenStahl et al
Radiology
TABLE 7 Cost-Effectiveness of NINDS-compliant Strategy as Compared with Current Clinical Practice Intervention
Average Total Cost per Patient ($)*
Total Effectiveness (QALY)*
Incremental Cost ($)
Incremental Effectiveness (QALY)
Cost-Effectiveness ($)†
Current clinical practice NINDS-compliant practice
69,539 69,105
3.63 3.64
⫺434‡
0.01
⫺52,609
* Costs and effects are for all persons combined (ie, those treated and those not treated with tPA) in a strategy. The discount rate was 3%. † Incremental cost divided by incremental effectiveness. ‡ When a strategy is more effective and less costly than the competing strategy, it is considered “dominant.”
Figure 3. Graph shows average QALYs (for 10,000 patients presenting with stroke symptoms) versus number of patients competing for CT per day.
Figure 4. Graph shows time from emergency arrival to treatment for patients with stroke versus number of patients competing for CT per day.
tation. The NINDS-compliant strategy remained cost saving for expenditures of up to $230 per presenting patient with stroke and remained cost-effective (at less than $50,000 per QALY) for up to $450 spent per patient presenting with stroke symptoms. This toll per patient is relative to the cost of current practice. This senVolume 228
䡠
Number 3
sitivity is due to the fact that this cost per patient is spent to achieve only a small increment in expected QALYs for society as a whole. Reducing the time from stroke onset to emergency department arrival or extending the window of therapeutic opportunity also had a large effect. Assuming the performance of the current system, any strategy that either reduces the arrival interval by 30 minutes or lengthens the time available for treatment by 30 minutes would result in between 4.1% and 7.7% of patients with stroke receiving treatment in time—three to six times, respectively, the number of patients currently treated. Such strategies would be cost saving for up to $100 per patient presenting with stroke symptoms and would remain cost-effective (at less than $50,000 per QALY) for spending up to $315 per patient presenting with stroke symptoms. The time needed to complete a task and the number of units available to perform a task have similar but not identical effects on the performance of a system. Reducing the time from emergency department arrival to CT scanning to 5 minutes increased the number of treatable patients from 1.4% to 1.8%. Reducing the time needed to interpret CT results to 5 minutes did not appear to substantially increase or reduce the number of patients treated, except in conditions in which CT scanners were running nonstop. Increasing the number of CT scanners was more effective. Increasing the number of available CT scanners from two to eight in the current practice environment resulted in a 7% increase (from 1.4% to 1.5%) in the number of treatable patients, with an average gain in QALYs of 3.6272–3.6273 for all patients presenting with stroke symptoms. Increasing the number of available neurologists to more than four had less effect in a nonsaturated environment and increased the proportion of treatable patients from 1.43% to 1.44%. Neurologists had the greatest effect in situations in
which there were a high volume of patients with stroke and the CT scanners were already “saturated”—for instance, in a scenario in which there were two CT scanners, 60 nonstroke patients per day, and 10 patients with stroke per day. In this case, the relative gain in the number of treatable patients resulting from doubling CT capacity is 4.4%; the relative gain from doubling the number of neurologists, 6.3%; and the relative gain from doubling both, 9.1%. In our institution, Massachusetts General Hospital, approximately 60 patients per day are examined with the emergency department CT scanners. With the current strategy, with 1.4% of patients arriving in time to be treated and two CT scanners available, competition from nonstroke patients for the CT resource has a modest effect on patient outcome until the number of nonstroke patients approaches 120 per day (ie, five patients per hour), at which point stroke patients have substantial difficulty in having timely access to the CT scanners (Figs 3, 4). With current capacity constraints, the current system could not accommodate more than 7.5 stroke patients per day before patients began not to receive treatment owing to delays within the system.
DISCUSSION Most other cost-effectiveness analyses in which the role of tPA has been examined have been focused on the cost-effectiveness of tPA in those treated versus those not treated rather than on the cost-effectiveness of improving the efficiency of the process of evaluation and treatment. Results of each of these analyses (38,40,55,76) show thrombolytic therapy to be cost-effective or cost saving. This is in accordance with our own results, in which the quality-adjusted life expectancy of individual stroke patients who present within 3 hours of stroke onset increased, on average, from 3.62 to 3.99 QALYs at reasonable cost. The few prospective studies of the delivery of care
Implementing a Stroke Protocol Compliant with NINDS Recommendations
䡠
665
Radiology
have mostly been focused on evaluating single interventions such as code beepers (36), cellular phones for emergency medical services personnel (77,78), and providing more specialist care at hospital arrival (79). The largest examination of the stroke care process was the pretrial total quality improvement effort performed by the NINDS stroke study group (39). Unfortunately, it is difficult to determine the effect of this effort, because performance data prior to the total quality improvement effort in 1991 are not available. Results of our analysis also show that implementing a stroke evaluation and management system that is compliant with NINDS recommendations would be cost-effective and probably cost saving to society as a whole. The relatively small gain is due to the QALY gain for a few patients receiving treatment in time being considered across 10,000 patients. Therapy is only useful if the patient receives it in time for it to be effective. A NINDS-compliant stroke team and system shortens the time needed for the evaluation and care of patients with stroke and potentially reduces the variance in the delivery of care. Use of such a system should more than double the number of patients that can be treated. The next question is: Can we afford to do this? Although previously published reports (39) have suggested that administrative and policy process improvements in stroke care might be implemented without significant investment of capital, we believed that we could not a priori make the assumption that implementing a NINDS-compliant strategy was costless. By the same token, we believed we could not know ahead of time the capital resources already available to hospital systems across the country or the investments, such as purchasing an additional CT scanner, that may or may not be needed for a hospital to become NINDS compliant. On the basis of expert opinion (J.E.S., S.G., K.L.F.), we made what we believed to be both a reasonable and conservative assumption as to a capital base of two CT scanners for a busy city hospital. We also assumed that any additional investment toward implementing this guideline would be in the form of manpower. This was reaffirmed when we explored the effect of CT scanner availability through sensitivity analyses. The effectiveness of the strategies were relatively insensitive to the number of available CT scanners except at very high vol666
䡠
Radiology
䡠
September 2003
umes of patients. This implies that, for most hospitals, investing in an additional CT scanner is not necessary to become NINDS compliant. The time spent in the CT scanner, approximately 10 minutes, is too short for it to become a significant bottleneck unless general patient demand for a CT scanner exceeds 60 patients per day per scanner or unless stroke prevalence is four to five times the national average. Both are unlikely in smaller hospitals. Therefore, the CT scanner is not the main roadblock toward achieving NINDS compliance; rather, NINDS compliance in lower-volume conditions is most dependent on staffing and on managing the time needed for triage and clinical evaluation of patients. Because the cost of implementation is not knowable a priori, when one is exploring the cost of becoming NINDS compliant compared with the cost of current practice, the question has to be framed as, “How much must implementing a NINDS-compliant system cost before the cost outweighs its benefits?” Through sensitivity analysis we added overhead costs for all patients, both treated and not treated, presenting for evaluation for stroke in a NINDS-compliant strategy. Even assuming an additional overhead cost of $450 per patient presenting with stroke symptoms, a NINDS-compliant protocol was both cost-effective and inexpensive relative to other health interventions (80). In other words, if one assumes that, on average, 1.75 patients present with stroke symptoms per day at a busy city hospital emergency department, then complying with the NINDS recommendations would require that an additional $290,000 per year, spread across 640 patients, be spent. Although there is no absolute threshold for determining whether or not a therapeutic intervention is cost-effective, up to $100,000 per life year per person is generally considered to be acceptable (33,81,82). Because the mean time from stroke onset to arrival, 3.11 hours, is higher than though close to the limit of the window of therapeutic opportunity, the effectiveness of any system for delivering care is extremely sensitive to the time needed to implement each element in the care process. This is the main reason why a NINDS-compliant strategy is so cost-effective even when assuming a substantial cost per patient. Unfortunately, a NINDS-compliant strategy only addresses the easiest-tocontrol aspect of stroke care—the process times within a hospital. Even if we carefully control the time spent evaluating
and treating patients within the hospital, we are still only reaching a small segment of the population with stroke. Even if we reduce the time the emergency medicine physician and neurologist spend with the patient, the time needed to image the patient and deliver thrombolytics can only be reduced so far. The biggest gain would be from any intervention that expands the therapeutic window or from any intervention that reduces the time from stroke onset to arrival, such as public awareness campaigns (eg, that sponsored by the Brain Attack Coalition [www.stroke-site.org]) (20,44) that make potential stroke victims more aware of the symptoms and signs of stroke as well as the need for emergent medical care. Any strategy in which arrival time is reduced or the therapeutic window is increased by 30 minutes while less than $315 is spent per patient with stroke should be justifiable from a societal perspective. It should be noted, however, that new interventional radiologic techniques such as those being pioneered in the Prolyse in Acute Cerebral Thromboembolism (PROACT) II trial (16) may also be valuable to pursue because they may widen the window of therapeutic opportunity. Outcome studies based on the results of these trials may help determine the value of these techniques. Results of our analysis also show that although a stroke center is sensitive to the volume of nonstroke patients competing for CT and emergency medicine physician time, it is most sensitive to the volume of patients presenting with stroke symptoms. This is because patients with stroke require both CT and neurologist time almost simultaneously. CT capacity appears to be a greater bottleneck than the number of available neurologists. Because the CT process is relatively short, very large volumes—twice the current volume at our center—are required to overload the CT scanning process to the point that delays due to CT scanner availability and neurologist availability in and of themselves significantly reduce the number of patients that might be treated. This is not true for centers with only one CT scanner. Results of our analysis therefore imply that at a high-volume stroke center, there should be at least two CT scanners and four neurologists available. The NINDS and other organizations have made recommendations as to how to best treat patients with stroke in a timely fashion. This effort has had two main foci: First, educating the public to recognize and act on stroke symptoms, Stahl et al
Radiology
and second, improving the speed with which patients are treated once they arrive at the hospital. Our results show that, as might be expected, both reducing the time from symptom onset to emergency department arrival and reducing the time from emergency department arrival to treatment would improve outcomes for stroke patients. A result that might not have been expected is that introducing such an in-hospital protocol would not only be cost-effective over a wide range of conditions but would also probably be cost saving. Undoubtedly, reducing in-hospital time to treatment is a worthwhile goal and is probably easier to achieve than reducing the time from stroke onset to emergency department arrival. But because so much time is wasted from stroke onset to presentation at the emergency department, the potential gains from educating the public to recognize and act on stroke symptoms more quickly may in the long run be greater. One of the most important limitations in this study was the limited availability of raw timing data on all aspects of the clinical process. Relatively few studies have been focused on the process of care as the primary concern, and these data are not readily available. Another limitation was that there are few data to guide the estimation of the cost of becoming NINDS compliant and hence the sensitivity analysis of the cost per patient presenting with stroke symptoms. Another potential limitation was environmental. There is some evidence of a secular trend toward reduction in the time from arrival to therapy (83). This may have resulted in the benefit of instituting a NINDScompliant system having been overestimated in the model. Finally, the use of potential tissue-sparing medications such as nifedipine was not specifically modeled, although most of the effect of the use of such medications was captured through sensitivity analyses in which the therapeutic window was extended. References 1. U.S. Department of Health and Human Services. Current estimates from the National Health Interview Survey, 1995: vital and health statistics. Series 10: Data From the National Health Survey No. 199, 1998. 2. Rosamond W, Folsom A, Chambless L, et al. Stroke incidence and survival among middle-aged adults: 9-year follow-up of the Atherosclerosis Risk in Communities (ARIC) cohort. Stroke 1999; 30:736 –743. 3. McCaig, LF, Burt CW. National Hospital Ambulatory Medical Care Survey: 1999 emergency department summary. AdVolume 228
䡠
Number 3
4. 5.
6.
7. 8.
9.
10.
11.
12.
13.
14. 15.
16.
17.
18.
19.
20.
vance Data from Vital and Health Statistics No. 320. Hyattsville, Md: National Center for Health Statistics; 2001. American Heart Association. 1999 Heart and Stroke Statistical Update. Dallas, Tex: American Heart Association, 1998. Metropolitan Life Insurance Company. 1999 heart and stroke statistical update: statistical bulletin. New York, NY: Metropolitan Life Insurance Company, 1997. Leibson C, Brown RD, Hass SL, O’Fallon WM, Whisnant JP. Utilization of acute care services in the year before and after first stroke: a population-based study. Neurology 1996; 46:861– 869. Rankin J. Cerebral vascular accidents in patients over 60. II. Prognosis. Scott Med J 1957; 2:200 –215. Thrombolytic therapy with streptokinase in acute ischemic stroke: the Multicenter Acute Stroke Trial—Europe Study Group. N Engl J Med 1996; 335:145–150. Donnan G, Davis S, Chambers B, et al. Streptokinase for acute ischemic stroke with relationship to time of administration: Australian Streptokinase (ASK) Trial Study Group. JAMA 1996; 276:961–969. Tissue plasminogen activator for acute stroke: the National Institute of Neurological Disorders and Stroke rt-PA Stroke Study Group. N Engl J Med 1995; 333: 1581–1587. Hacke W, Kaste M, Fieschi C. Intravenous thrombolysis with recombinant tissue plasminogen activator for acute hemispheric stroke: the European Cooperative Acute Stroke Study (ECASS). JAMA 1995; 274:1017–1025. Randomised controlled trial of streptokinase, aspirin, and combination of both in treatment of acute ischaemic stroke: Multicentre Acute Stroke Trial—Italy (MAST-I) Group. Lancet 1995; 346:1509 –1514. Lyden P, Brott T, Tilley B, et al. Improved reliability of the NIH Stroke Scale using video training: NINDS TPA Stroke Study Group. Stroke 1994; 25:2220 –2226. Mahoney F, Barthel D. Functional evaluation: the Barthel Index. Md Med J 1965; 61– 65. Teasdale G, Knill-Jones R, van der Sande J. Observer variability in assessing impaired consciousness and coma. J Neurol Neurosurg Psychiatry 1978; 41:603– 610. Furlan A, Higashida R, Wechsler L, et al. Intra-arterial prourokinase for acute ischemic stroke: the PROACT II study—a randomized controlled trial. Prolyse in acute cerebral thromboembolism. JAMA 1999; 282:2003–2011. Rosamond W, Gorton R, Hinn A, Hohenhaus S, Morris D. Rapid response to stroke symptoms: the Delay in Accessing Stroke Healthcare (DASH) study. Ann Emerg Med 1998; 5:45–51. Wester P, Radberg J, Lundgren B, Peltonen M. Factors associated with delayed admission to hospital and in-hospital delays in acute stroke and TIA: a prospective, multicenter study—Seek-MedicalAttention-in-Time Study Group. Stroke 1999; 30:40 – 48. Williams J, Rosamond W, Morris D. Stroke symptom attribution and time to emergency department arrival: the delay in accessing stroke healthcare study. Acad Emerg Med 2000; 7:93–96. Proceedings of a National Symposium on
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
34. 35. 36.
37.
Rapid Identification and Treatment of Acute Stroke. Vol 2001. Bethesda, Md: National Institute of Neurological Disorders and Stroke, 1996. Smith M, Doliszny K, Shahar E, McGovern P, Arnett D, Luepker R. Delayed hospital arrival for acute stroke: the Minnesota Stroke Survey. Ann Intern Med 1998; 129:190 –196. Morris D, Rosamond W, Hinn A, Gorton R. Time delays in accessing stroke care in the emergency department. Acad Emerg Med 1999; 6:218 –223. Lacy CR, Suh DC, Bueno M, Kostis JB. Delay in presentation and evaluation for acute stroke: Stroke Time Registry for Outcomes Knowledge and Epidemiology (S.T.R.O.K.E.). Stroke 2001; 32:63– 69. Azzimondi G, Bassein L, Fiorani L, et al. Variables associated with hospital arrival time after stroke. Stroke 1997; 28:537– 542. Fodelholm R, Murros K, Rissanen A, Ilmavirta M. Factors delaying hospital admission after acute stroke. Stroke 1996; 27: 398 – 400. Kothari R, Jauch E, Broderick J, et al. Acute stroke: delays to presentation and emergency department evaluation. Ann Emerg Med 1999; 33:3– 8. Morris D, Rosamond W, Madden K, Schultz C, Hamilton S. Prehospital and emergency department delays after acute stroke: the Genentech Stroke Presentation Survey. Stroke 2000; 31:2585–2590. Schroeder E, Rosamond W, Morris D, Evenson K, Hinn A. Determinants of use of emergency medical services in a population with stroke symptoms. Stroke 2000; 31:2591–2596. Smith R, Scott P, Grant R, Chudnofsky C, Frederiksen S. Emergency physician treatment of acute stroke with recombinant tissue plasminogen activator: a retrospective analysis. Ann Emerg Med 1999; 6:618 – 625. Hacke W, Kaste M, Fieschi C, et al. Randomised double-blind placebo-controlled trial of thrombolytic therapy with intravenous alteplase in acute ischaemic stroke (ECASS II). Lancet 1998; 352:1245– 1251. Streifler J, Davidovitch S, Sendovski U. Factors associated with the time of presentation of acute stroke patients in an Israeli community hospital. Neuroepidemiology 1998; 17:161–166. Proceedings of a National Symposium on Rapid Identification and Treatment of Acute Stroke, National Institutes of Health, December 12–13, 1996. Bethesda, Md: National Institute of Neurological Disorders and Stroke. Gold MR, Siegel JE, Russel LB, Weinstein MC. Cost-effectiveness in health and medicine. New York, NY: Oxford University Press, 1996; 425. Banks J. Handbook of simulation. New York, NY: Wiley, 1998. Law A, Kelton D. Simulation modeling and analysis. New York, NY: McGrawHill, 1991. Gomez C, Malkoff M, Sauer C, Tulyapronchote R, Burch C, Banet G. Code stroke: an attempt to shorten inhospital therapeutic delays. Stroke 1994; 25:19201923. Jorgensen H, Nakayama H, Raaschou H.
Implementing a Stroke Protocol Compliant with NINDS Recommendations
䡠
667
Radiology
38.
39.
40.
41. 42.
43.
44.
45.
46. 47.
48.
49. 50.
668
The effect of a stroke unit: reductions in mortality, discharge rate to nursing home, length of hospital stay, and cost—a community-based study. Stroke 1995; 26:1178 –1182. Lanzieri C, Tarr R, Landis D, et al. Costeffectiveness of emergency intraarterial intracerebral thrombolysis: a pilot study. AJNR Am J Neuroradiol 1995; 16:1987– 1993. Tilley B, Lyden P, Brott T, Lu M, Levine S, Welch K. Total quality improvement method for reduction of delays between emergency department admission and treatment of acute ischemic stroke: the National Institute of Neurological Disorders and Stroke rt-PA Stroke Study Group. Arch Neurol 1997; 54:1466 –1474. Wein T, Hickenbottom S, Alexandrov A. Thrombolysis, stroke units and other strategies for reducing acute stroke costs. Pharmacoeconomics 1998; 14:603– 611. Alberts M, Bertels C, Dawson D. An analysis of time of presentation after stroke. JAMA 1990; 263:65– 68. Davalos A, Castillo J, Martinez-Vila E. Delay in neurological attention and stroke outcome: Cerebrovascular Diseases Study Group of the Spanish Society of Neurology. Stroke 1995; 26:2233–2237. O’Connor R, McGraw P, Edelsohn L. Thrombolytic therapy for acute ischemic stroke: why the majority of patients remain ineligible for treatment. Ann Emerg Med 1999; 33:9 –14. Adams HP Jr, Brott TG, Furlan AJ, et al. Guidelines for thrombolytic therapy for acute stroke: a supplement to the guidelines for the management of patients with acute ischemic stroke—a statement for healthcare professionals from a Special Writing Group of the Stroke Council, American Heart Association. Stroke 1996; 27:1711–1718. Mayberg M, Batjer H, Dacey R, et al. Guidelines for the management of aneurysmal subarachnoid hemorrhage: a statement for healthcare professionals from a special writing group of the Stroke Council, American Heart Association. Circulation 1994; 90:2592–2605. Schievink W. Intracranial aneurysms. N Engl J Med 1997; 336:28 – 40. Ambulatory care visits to physician offices, hospital outpatient departments, and emergency departments: United States, 1997. Hyattsville, Md: Vital and Health Statistics Series 13, No. 143. 1997; 13. Table 26: number of deaths, death rates, and age-adjusted death rates for major causes of death for the United States, each division, each state, Puerto Rico, Virgin Islands, Guam, American Samoa, and Northern Marianas, 1998 -. Hyattsville, Md: National Vital Statistics Reports, Vol 48, No. 11, July 24, 2000, 1998. Nussbaum ES, Heros RC, Erickson DL. Cost-effectiveness of carotid endarterectomy. Neurosurgery 1996; 37:237–244. Sacco SE, Whisnant JP, Broderick JP, Phillips SJ, O’Fallon WM. Epidemiological
䡠
Radiology
䡠
September 2003
51.
52.
53.
54. 55.
56.
57.
58. 59.
60.
61.
62.
63.
64.
65.
66. 67.
characteristics of lacunar infarcts in a population. Stroke 1991; 22:1236 –1241. Sacco R, Wolf P, Kannel W, McNamara P. Survival and recurrence following stroke: the Framingham Study. Stroke 1982; 13: 290 –295. Alexander M. Stroke rehabilitation outcome: a potential use of predictive variables to establish levels of care. Stroke 1994; 25:128 –134. Falconer J, Naughton B, Strasser D, Sinacore J. Stroke inpatient rehabilitation: a comparison across age groups. J Am Geriatr Soc 1994; 42:39 – 44. Granger C, Hamilton B, Fiedler R. Discharge outcome after stroke rehabilitation. Stroke 1992; 23:978 –982. Fagan S, Morgenstern L, Petitta A, et al. Cost-effectiveness of tissue plasminogen activator for acute ischemic stroke. Neurology 1998; 50:883– 890. Mark D, Hlatky M, Califf R, et al. Costeffectiveness of thrombolytic therapy with tissue plasminogen activator as compared to streptokinase for acute myocardial infarction. N Engl J Med 1995; 332:1418 –1424. Solomon N, Glick H, Russo C, Lee J, Schulman K. Patient preferences for stroke outcomes. Stroke 1994; 25:1721– 1725. Tengs TO, Yu M, Luistro E. Health-related quality of life after stroke: a comprehensive review. Stroke 2001; 32:964 –972. Gage B, Cardinalli A, Owens D. The effect of stroke and stroke prophylaxis with aspirin or warfarin on quality of life. Arch Intern Med 1996; 156:1829 –1836. Duncan P, Lai S, Keighley J. Defining post-stroke recovery: implications for design and interpretation of drug trials. Neuropharmacology 2000; 39:835– 841. Hallan S, Asberg A, Indredavik B, Wideroe T. Quality of life after cerebrovascular stroke: a systematic study of patients’ preferences for different functional outcomes. J Intern Med 1999; 246:309 –316. Post P, Stiggelbout A, Wakker P. The utility of health states after stroke: a systematic review of the literature. Stroke 2001; 32:1425–1429. Aoki N, Kitahara T, Fukui T, Beck J, Soma K, Yamamoto W. Management of unruptured intracranial aneurysm in Japan: a Markovian decision analysis with utility measurements based on the Glasgow coma scale. Med Decis Making 1998; 18: 357–364. King J, Glick H, Mason T, Flamm E. Elective surgery for asymptomatic, unruptured intracranial aneurysms: a cost-effectiveness analysis. J Neurosurg 1995; 83:403– 412. Holloway R, Witter D, Lawton K, Libscomb J, Samsa G. Inpatient costs of specific cerebrovascular events at five academic medical centers. Neurology 1996; 46:854 – 860. Staff ME. Red book. Montvale, NJ: Medical Economics, 2000; 800. Occupational outlook handbook: physicians and surgeons. U.S. Department of
68.
69.
70.
71.
72. 73.
74. 75. 76.
77.
78.
79.
80.
81.
82.
83.
Labor Bureau of Labor Statistics Web site. Available at: http://stats.bls.gov/oco/ ocos074.htm. Accessed June 16, 2003. Lee J, Huber J, Stason W. Poststroke rehabilitation in older Americans: the Medicare experience. Med Care 1996; 34:811– 825. Weiner J, Ilston L, Hanley R. Sharing the burden: strategies for public and private long-term insurance. Washington, DC: Brookings Institute, 1993. Sacco R, Shi T, Zamanillo M, Kargman D. Predictors of mortality and recurrence after hospitalized cerebral infarction in an urban community: the Northern Manhattan Stroke Study. Neurology 1994; 44: 626 – 634. Holloway R, Benesch C, Rahilly C, Courtright C. A systematic review of costeffectiveness research of stroke evaluation and treatment. Stroke 1999; 30: 1340 –1349. Home page. U.S. Department of Labor Bureau of Labor Statistics. Available at: www.bls.gov. Accessed June 16, 2003. Data warehouse home page. National Center for Health Statistics. Available at: www.cdc.gov/nchs/datawh/statab/unpubd/ mortabs.htm. Accessed June 16, 2003. Home page. U.S. Census Bureau. Available at: www.census.gov. Accessed June 16, 2003. Sox H, Blatt M, Higgins M, Marton K. Medical decision making. Newton, Mass: Butterworth-Heinemann, 1988. Hallan S, Asberg A, Indredavik B, Wideroe T. A decision analysis of thrombolytic therapy compared with standard therapy in acute ischaemic stroke. J Intern Med 1999; 246:549 –559. Brott T, Haley E, Levy D, Barsan W, Broderick J, Marler J. Thrombolytic therapy in acute ischemic stroke: strategies for early treatment of acute cerebral infarction. Berlin, Germany: Springer-Verlag, 1991; 197–203. Brott T, Haley E, Levy D. Urgent therapy for stroke. II. Pilot study of tissue plasminogen activator administered within 90 minutes. Stroke 1992; 23:632– 640. Kaste M, Palomaki H, Sarna S. Where and how should elderly stroke patients be treated? A randomized trial. Stroke 1995; 26:249 –253. Tengs T, Adams M, Pliskin J, et al. Fivehundred life-saving interventions and their cost-effectiveness. Risk Anal 1995; 15:369 –390. Azimi N, Welch H. The effectiveness of cost-effectiveness analysis in containing costs. J Gen Intern Med 1998; 13:664 – 669. Winkelmayer W, Weinstein M, Mittelman M, Glynn R, Pliskin J. Health economic evaluations: the special case of end-stage renal disease treatment. Med Decis Making 2002; 22:417– 430. Morgenstern LB, Staub L, Chan W, et al. Improving delivery of acute stroke therapy: the TLL Temple Foundation Stroke Project. Stroke 2002; 33:160 –166.
Stahl et al