The development and implementation of a taxonomy of case management in brain injury (BICM-T) -providing the answers to the questions Authors: Lukersmith, Sue ., Croker, Dianne ., Salvador-Carulla, Luis 1,3
3
1,2
Affiliations: 1. Faculty of Health Sciences, University of Sydney, Sydney, Australia 2. Brain and Mind Research Institute, University of Sydney, Sydney, Australia 3. Lifetime Care & Support Authority, Sydney, Australia
on behalf of the CM nominal group
BACKGROUND AND AIM:
RESULTS:
Community-based case management makes a unique contribution towards the improved functioning and community participation of people with complex health conditions such as brain injury [1-3].
What does the taxonomy involve?
How come there is no international consensus on what is, and what is not case management? Case management necessarily involves complexities and variability associated with the services, interpretations of roles and responsibilities as well as client circumstances and context. There are multiple components to consider. Each country, organisation and service has their own ‘model’ of case management depending on the context and the client’s health condition. Case management occurs in populations with such diverse health conditions as diabetes, malaria, dementia, HIV, stroke, mental health and brain injury. Case managers from different health disciplines bring slightly different approaches to their work.
The BICM-T is a multi-dimensional framework and considers factors related to the case management service domains and a taxonomy tree of key components (interventions or actions). It includes a consensus definition of case management and glossary of terms. The definition of case management in the BICM-T is Community-based case management - Community-based case management is a multidimensional and collaborative process. It involves a set of interventions for assessment, planning, coordinating and review of the options and services required to meet the client’s health-related needs, and support them to reach their goals related to participation in life roles Lukersmith, S., Fernandez, A., Millington, M., CM Nominal Group, Salvador-Carulla, L. (2015) The Glossary: A preliminary taxonomy of community-based case management in brain injury (BICM-PT)
Case managers performing one or a number of case management interventions are often called by many different names. To mention a few: Community care coordinator, care coordinator, case monitor, coordinator, local area planner, discharge planner, support broker, support facilitator and support navigator. Case management is not a discipline rather is set of interventions.
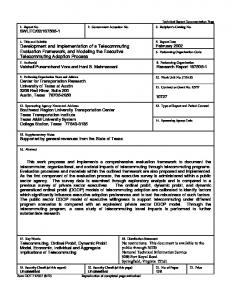
Only the intervention tree is presented here (Refer to Figure 1 below). Contact the first author for the glossary of terms, service tree and intervention and service tables.
Further, not all case managers perform all of the same interventions. They do not work for the same types of organisations and services, nor within the same jurisdictions.
Organisations such as the Lifetime Care and Support Authority (LTCS) will be able to use the taxonomy to enhance communication, understanding and business practices over the coming years to:
A quintessential Asian phrase used to explain similarities but differences “same same but different” is also true of case management. Why is that a problem? The variability of case management is a problem for research on case management effectiveness. There have been numerous systematic reviews [4, 5] and studies [6, 7] which highlight the difficulties with clinical trials, the heterogeneity between interventions, the range of outcomes measured and the association between case management components or interventions and client outcomes. The lack of a common language on case management has a subsequent impact on quality analysis, policy development, planning and funding of services, as well as management of, and training for case managers.
How will it be used?
࢚࢚ Promote better understanding between stakeholders including service providers, clients and organisations about what is and what is not case management. Enhanced language and understanding supports problem solving between stakeholders. ࢚࢚ Explore the different roles and the expectations for case management activities particularly with respect to clients in the post-acute phase following serious injury compared to clients who are many years post injury. ࢚࢚ Distinguish between different case management services and their strengths ࢚࢚ Strengthen training and mentoring opportunities including the development of training resources ࢚࢚ Link case management interventions with outcomes. If what is being done is better understood, then specific components of case management can be linked to improved outcomes. As other organisations and researchers in Australia and other countries become aware of the taxonomy, additional applications of the taxonomy in different contexts are emerging.
What is the solution? The aim was to develop a knowledge framework (the taxonomy) and common language for researchers and organisations like the Lifetime Care & Support Authority (LTCSA) and other stakeholders to support quality analysis, best practice, skill development and training.
Conclusions: The taxonomy is a knowledge to practice tool. It provides a common language for case management practitioners, services and funding organisations relevant for monitoring, comparisons, business planning and quality assessment. Figure 1. Interventions (throughputs) tree
METHODS
Taxonomy tree for community-based case management in brain injury (BICM-T) Interventions (throughputs)
Main Actions (parent categories) Engagement
What is a taxonomy? A taxonomy is a type of knowledge map and framing tool that uses a common language. As a classification structure, a taxonomy organises knowledge and articulates the relationship between concepts and components, and provides definitions [8, 9].
Actions (child categories)
Related Actions
Acceptance of referral Establish partnerships
Holistic Assessment
Ascertain capacity for decision making
Listening Observation Test Gathering information from other sources
How did we develop the taxonomy?
Measurement of outcomes
The study used mixed qualitative research methods over 18 months to develop the taxonomy. The methods included a scoping study and critical review of international frames to develop the Beta 1 version. A nominal group technique used with a group of case management experts followed (refer to Table 1). The expert knowledge across the group included brain injury case management practice (adults and children), policy, planning, management and funding. It had representation from public, private and not for profit sectors, included different health disciplines and experts from both urban and rural settings. There were meetings over 6 months for refinement into the Beta 2 version. After a feasibility analysis using case studies and a review of the alignment to the international frames and a final nominal group meeting, the BICM-T was finalised in January 2015.
Planning
Preparation Facilitation and support of client planning
Education
Provide decision making supports
Planning long term supports
Training & Skills Development
Navigating
Linking
Facilitating
Client support - task performed
Advocating
Client support - practical support
Collaboration & consultation
Resolution of issues
Case consultation
Building knowledge
Coordination
Maintaining feedback
Bridging
Monitoring
Managing documentation
Emotional & Motivational Support
Advising
Lukersmith, S., Fernandez, A., Millington, M., Salvador-Carulla, L., on behalf of the CM Nominal Group (2015). A taxonomy of community-based case management in brain injury.
Table 1. Case management experts
References:
Areas of expert knowledge Name
Professional background
1
Di Croker
Occupational therapy
2
Margaret Doyle
3
Client group*
Case Management
Service Context +
Geographic ++
Practice
Policy Planning
Management
Funding
A
X
X
X
X
Speech pathology
A
X
X
X
Pub
U
Marion Fisher
Speech pathology
C
X
X
X
Pub, Pr
U
4
Rebbekah Loukas
Psychology
A
X
X
X
NFP
U
5
Suzanne Lulham
Physiotherapy & law
B
X
X
6
Elizabeth Shannon
Physiotherapy
A
X
7
Jo Suhanic
Social work
B
X
X
8
Deb Toffolo
Speech pathology
B
X
X
9
Karen Williams
Nursing
B
X
10 Janine Wood
Speech pathology
B
X
X
11 Denise Young
Social work
B
X
X
X
12 Sue Lukersmith^
Occupational therapy
B
X
X
X
^ Facilitator
* Client Group: Adult=A, Children=C, Both Adult and Children=B # CM practice: Practice, Policy and planning, Management, Funding + Service context: Public (Pub), Private (Pr), Not-for profit (NFP). ++ Geographic; Urban (U) rural (R)
X
2. Pub, Pr
Pub, Pr Pr Pub
X
X
1.
U,R
U,R U U,R
Pr
U
Pr
R
Pub
U,R
Pub
R
Pub, Pr
U
3. 4. 5. 6. 7. 8. 9.
Khan, F., I. Baguley, and I. Cameron, Rehabilitation after traumatic brain injury Medical Journal of Australia, 2003. 178(17 March ): p. 290-295. Alli, C., et al., Clinical inquiries. Does case management improve diabetes outcomes? Journal of Family Practice, 2008. 57(11): p. 747-8. Brombley, K., Better at home? Benefits of case management for children with complex needs. Paediatric Nursing, 2008. 20(9): p. 24-6. Reilly, S., et al., Case management approaches to home support for people with dementia (Review). Cochrane Database of Systematic Reviews, 2015(1). Kopke, S. and J. McCleery, Systematic reviews of case management: too complex to manage? (editorial). Cochrane Database of Systematic Reviews, 2015. 1(ED000096). Lannin, N., et al., An Australian Survey of the Clinical Practice Pattersn of Case Management for Clients with Brain Injury. Brain Impairment 2012. 13(2): p. 228-237. Fitzsimmons, R.D., Brain injury case management: the potential and limitations of latestage intervention--a pilot study. Brain Injury, 2003. 17(11): p. 947-71. Salvador-Carulla, L., et al., Framing of scientific knowledge as a new category of health care research. J Eval Clin Pract, 2014. 20(6): p. 1045-55. Lambe, P., Organising knowledge: Taxonomies, knowledge and organisational effectiveness 2007, Oxford Chandos publishing
For further information contact Sue Lukersmith email:
[email protected] or
[email protected]