The effects of protein synthesis inhibitors and the lysosomotropic agent chloroquine on the metabolism of the insulin receptor were examined. Through the use.
Vol. 260, No. 26, Issue of November 15,pp. 14180-14188,1985 Printed in U.S.A.
THEJOURNAL OF B~OLOCICAL CHEMISTRY 0 1985 byThe American Society of Biological Chemists, Inc.
The Effects of Cycloheximide and Chloroquine on Insulin Receptor Metabolism DIFFERENTIALEFFECTS DEGRADATION*
ON RECEPTOR RECYCLING AND INACTIVATION AND INSULIN
(Received for publication, May 22,1985)
Victoria P. KnutsonS, Gabriele V. Ronnettt, andM.Daniel Lane From the Department of Biological Chemistry, The Johns Hopkins University School of Medicine, Baltimore, Maryland 21205
The effects of protein synthesis inhibitors and the ferent rates, butpossibly occur in distinct subcellular lysosomotropic agent chloroquineon the metabolism of locations. the insulin receptor were examined. Through the use of the heavy-isotope density shifttechnique, cycloheximide was found to inhibit both the synthesis of new The insulin receptor is a metabolically dynamic protein insulin receptor and the inactivation of old cellular insulin receptor.Upon investigation of the locus of this whose cellular steady state level can be attenuated by various it was found that perturbants. Insulin itself decreases the basal cellular level of effect of protein synthesis inhibition, cycloheximide did not inhibit 1) the translocation of insulin receptor through a process known as ligand-induced receptor from the cell surface to an intracellular site, down-regulation. Extensive metabolic characterization of the 2) the recycling of receptor from the internal site back down-regulation process has been performed in cell culture to the plasma membrane, nor 3) the degradation of with 3T3-C2 mouse fibroblasts (1)and 3T3-Lladipocytes (2), insulin. Cycloheximidedid,however, rapidly andcom- demonstrating that in the steady state, down-regulation is pletely inhibit the inactivationof the insulinreceptor. associated with an increased rate constant for receptor inacIn the presence of extracellular insulin, thiseffect of tivation, with no change in the rate of receptor synthesis. cycloheximide resulted in the long-term(6 h) accumu- However, inhibition of general protein synthesisby cyclohexlation of receptor in a trypsin-resistant intracellular imide has been reported either to completely inhibit insulincompartment. Puromycinand pactamycin, protein induced down-regulation (3) or to markedly decrease the rate synthesis inhibitors withmechanisms of action which differ from cycloheximide, produced the same effects and extent of the down-regulation process (4,5). Cyclohexion insulin receptor metabolism as cycloheximide, in- mide has been shown to have similar effects on the liganddicating that thiseffect on receptor metabolism is due induced down-regulation of thyrotropin-releasing hormone to the inhibition of protein synthesis andnot a second- receptors (6) and luteinizing hormone receptors (7). To furary effect of cycloheximide. Actinomycin D also inhib- ther define the metabolic processing of the insulin receptor, studies were conducted to discern how inhibitors of protein ited the inactivationof receptor. Chloroquine inhibited the receptor-mediated degra- synthesis could inhibit the down-regulation process, a process dation of insulin, but hadno effect on either the inter- achieved and maintainedby accelerated receptor inactivation. nalization or inactivation of the insulin receptor. The Recent advances in assessing the rapid insulin-induced transinsulin-induced recycling of the internalized receptor location of insulin receptor from the cell surface to an intrawas inhibited bychloroquine, possibly through the in- cellular site (8) make it possible to localize the step(s) at hibition of the discharge of insulin from the insulin- which cycloheximideperturbs normal processing of the recepreceptor complex. tor. From these observations, we suggest that 1) a protein The lysosomotropic agent chloroquine has also been refactor is required to inactivate the insulin receptor, 2) ported to inhibit the normal metabolic processing of both this protein and the messenger RNA coding for the insulin and theinsulin receptor by inhibiting their lysosomal protein have short cellular half-lives, and 3) insulin degradation (9, 10). However, in a study utilizing cultured degradation and insulin receptor inactivationare dis- hepatocytes, chloroquine inhibited insulin degradation but tinct, separable processes which not only occur at dif- had no effect on receptor inactivation (11).This latterfinding suggests that while the insulin receptor and its bound ligand are endocytosed together, the catabolic processing of ligand * This investigation was supported by National Institutes of Health and receptor diverge at a point preceding lysosomal degradaGrant AM 14574 and by a grant from the Kroc Foundation. The tion. We provide strong evidence in this report, through the costs of publication of this article were defrayed in part by the use of cycloheximide and chloroquine, which indicates that payment ofpage charges. This articlemust therefore be hereby the intracellular processing of insulin and itsreceptor occurs marked “aduertisement” in accordance with 18 U.S.C. Section 1734 independently after internalization. solely to indicate this fact. f Supported by Postdoctoral Fellowship AM06609 from the National Institutes of Health. Current address: Department of Pharmacology, University of Texas Health Science Center at Houston, Medical School, Houston, T X 77030. 5 Supported in part by National Institutes of Health Medical Scientist Training Program Grant GM 07309 and the Juvenile Diabetes Foundation.
MATERIALS AND METHODS
Cell Culture-Mouse fibroblast 3T3-C2 cells were propagated and maintainedin monolayer culture as previously described (1).All experiments were conducted 18-24 h after a media change. Assays-Cell monolayers (6- or 10-cm culture dishes) were removed from the incubator, and media were aspirated from the dishes and
14180
Divergent CatabolicProcessing of Insulin and Insulin Receptor replaced with an equal volume of Krebs-Ringer phosphate buffer containing 1%bovine serum albumin. This wash was repeated twice, and the monolayers were incubated at 37 "C for 20 min. The buffer was then aspirated from the monolayers, and the wash/incubation procedure was repeated twice. The monolayers were then equilibrated to 4 "C. This wash procedure (referred to as the ligand debinding protocol) removed insulin boundto thecell surface and serum factors from the monolayers (1, 2). 1251-Labeledinsulin was prepared by the chloramine-T procedure (12) to a specific activity of 1 pCi/pmol, utilizing carrier-free NalZ5I (Amersham Corp.) and porcine insulin (Lilly). Cell surface insulin binding was assessed at 4 "C by aspirating the buffer from the monolayers and replacing it with 0.6 nM '"1insulin in phosphate-buffered saline containing 0.1% bovine serum albumin. Nonspecific binding was determined in paired monolayers by the addition of 3 p~ unlabeled insulin to the 0.6 nM 1261-insulin. Surface binding was allowedto equilibrate at least 6 h before washing the unbound insulin from the monolayers with 5 volumes of PBS,' 4 "C. Monolayers were dissolved with 1 N NaOH, and radioactivity was then quantitatedin a y-counter. Total solubilized receptor levels were determined as previously described (1). Briefly, monolayers were scraped from the dish into 50 mM Tris buffer (pH 7.4), containing 40 pl of Trasylol (FBA Pharmaceuticals, Inc., New York, NY) per ml of buffer. The cells were disrupted by homogenization and centrifuged at 100,OOO X g for 1h to obtain a total cellular membrane pellet. The insulin receptor was solubilized in theTris/Trasylol buffer containing 1%(w/v) Triton X-100 by homogenization and a 30-min 25 "C extraction. Nonsolubilized material was pelleted at 100,000 X g for 1 h. The resulting supernatant was assayed at 0.6 nM 1261-insulinat a final Triton X-100 concentration of 0.1%. Nonspecific binding was determined with3 PM unlabeled insulin. Binding, performed a t 4 "C, was carried out for 18 h, and bound and free insulin were separated by polyethylene glycol precipitation (13). All assays included both total andnonspecific binding and were performed in atleast duplicate in each experiment. Protein Synthesis Inhibitors-Stock solutions of cycloheximideand puromycin (Sigma) were prepared as 100-fold concentrated stock solutions in PBS immediately before use. Pactamycin (the generous gift of Dr. Joseph Grady, The Upjohn Co.) was also prepared immediately before use as a 100-fold concentrated ethanolic solution. At the concentrations of inhibitors utilized, protein synthesiswas inhibited by greater than 97% as determined by ['H]leucine (New England Nuclear) incorporation into trichloroacetic acid-precipitable material. Actinomycin D (Calbiochem-Behring) was also prepared as a 100fold concentrated stock solution in PBS; at 0.8 PM levels, protein synthesis was inhibited by 18%. Purificqtion of "C-, 16N-, and 'H-Enriched Amino Acids and the Density Shift Protocol-The lyophilized cells of ChloreUapyrenoidosa (>95 mol % 13C-, 15N-,and 'H-enriched) were kindly provided by Dr. Thomas Whaley, Stable Isotope Resource, Los Alamos Scientific Laboratory, Los Alamos, NM. The algae (15 g) were disrupted with 230 ml of 19% (w/v) trichloroacetic acid with agitation for 30 min a t 70 "C. The mixture was cooled to 4 "C and centrifuged at 10,000 X g for 10 min. The supernatant was discarded, and trichloroacetic acid precipitation and centrifugation were repeated twice. Pigment removal and delipidation were performed by extracting the residue three times with 250 ml of ethanol/ethyl ether (2:1, v/v) followed by five extractions with 75 ml of ether. Following each extraction, the residue was isolated by vacuum filtration over Whatman No. 42 filter paper. After the final extraction, the last traces of ether were removed by vacuum desiccation at 40 "C for 1 h. The residue was hydrolyzed in 200 ml of constant boiling 6 N HCI at 100 "C for 18h in a sealed, heavy wall glass vessel. After hydrolysis, the mixture was cooled to 4 "C and centrifuged at 7000 X g for 20 min. The insoluble residue. was washed twice with 100 ml of water, and the washings were combined with the hydrolysate. The hydrochloric acid was removed from the hydrolysate by repeated (three to five times) concentration witha rotary evaporatorattached tq a KOH pellet trap. The lasttraces of HC1 were removed from the syrup by drying in a vaccum oven at 100 "C for approximately 3 h. The syrup was diluted to 125 ml with water, filtered, and applied to a freshly washed 5 X 50-cm column ofDowex 50-X2, 100-200 mesh, H+ form (Sigma), at a flow rate of 1ml/min. The column was washed with 1.3liters of water, and theamino acids were eluted with 3 N ammonium hydroxide. The column void volume (approximately 500 ml) was discarded, and the following 600-800 ml was collected. The abbreviation used is: PBS, phosphate-buffered saline.
14181
The eluate was repeatedly concentrated to dryness with the rotary evaporator to remove the Iast traces of ammonia. The syrup was diluted to 150 ml with water and lyophilized. The dry weight of the resulting powder was 6 g. The heavy-isotope density shift protocol utilizes 150 mg of the dense amino acids/100 rnl of amino acid-free culture media containing 10%calf serum and supplemented with tryptophan, cystine, and glutamine (1). Treatment of the cell monolayers with media containingdense amino acids and thesubsequent workup have been described (1). Proteolysis of Cell Surface Insulin Receptor-Two schemes were used to proteolyze cell surface insulin receptors and torender them incapable of binding insulin. Scheme 1has been previously reported (1) and was utilized when the intact monolayer was to be subjected to metabolic studies subsequent to proteolysis. Briefly, the monolayers were subjected to the ligand debinding protocol described above, but using serum-free cell culture media instead of Krebs-Ringer phosphate buffer containing 1%bovine serum albumin. After debinding, the cells were mildly proteolyzed with 2 ml of trypsin, 20 Fg/ml in PBS, for 20 min at 37 "C. The proteolysis was terminated by aspirating the trypsin-containing buffer and replacing it with cell culture media, 10% calf serum, and 60 pg ofsoybean trypsin inhibitor (Sigma) per ml of media plus other drugs or inhibitors, as dictated by the experiment. Utilizing this scheme, greater than 96% of the cell surface insulin binding capacity of the monolayer was lost, but the cells remained firmly attached to the culture dish (1).Scheme 2 was utilized when proteolysis was required immediately prior to the preparation of total cellular membranes @), In general, five monolayers on 100-mm culture dishes were quickly washed three times with 8 ml of PBS at 22 "C. To each monolayer was added 2 ml of trypsin in PBS, 0.5 mg/ml, for 5 min at 22 "C. The trypsin-containing buffer was aspirated from the dish and replaced with 5 ml of PBS containing 3 mg of soybean trypsin inhibitor. This quench buffer was then replaced with 50 mM Tris/TrasyIol, and the cells were scraped, homogenized, centrifuged, and extracted as described above for the preparation of detergent-solubilized receptor. Insulin Receptor Internalization and Recycling-The insulin-induced rapid redistribution of insulin receptor from the plasma membrane to an intracellular compartment was monitored as previously described (8). The effects of cycloheximide, chloroquine, and other agents on this process were examined by incubating the cell monolayers with the agents alone for 10-20 min before the addition of 1.7 pM insulin to the monolayers. At timed intervalsthereafter, the monolayers were proteolyzed according to Scheme 2 described above, homogenized, solubilized, and banded isopycnically on CsCl gradients. The receptor level quantitated from the gradients represented the level of intracellular receptor. Insulin Degradation-The ability of cell monolayers to degrade '251-insulin was determined by adding 2 ml of culture media containing 10% calf serum and 1'51-insulin to each 60-mm culture dish. After incubation at 37 "Cin the COZincubator, 1ml of media was removed from the dish and immediately chilled on ice. To each aliquot of media, 1 ml of 20% (w/v) trichloroacetic acid was added, mixed, and iced for 30 min. The samples were then centrifuged for 10 min at 4 "C at 4000 rpm in a Sorvoll HS-4 rotor. One milliliter of the supernatant was counted to assess the amount of 1251-insulindegraded. To determine the corresponding level of cell-associated radioactivity, the remaining 1 mlof 1251-insuIin-containingmedia was aspirated from the dish; the monolayer was quickly washed three times with 4 ml of ice-coldPBS, and themonolayer was dissolved in 1.5 ml of 1 N NaOH prior to counting in a y-counter. RESULTS
Effects of Protein Synthesis Inhibitors on Insulin Receptor Metabolism-Cell monolayers were incubated for varying periods of time with 20 pM cycloheximide, 200 pM puromycin, or 1 ~ L pactamycin. M Atthese concentrations, proteinsynthesis was inhibited by at least 97%, as determinedby the incorporation of [3H]leucineinto trichloroacetic acid-precipitable protein. To further demonstrate that insulin receptor was not synthesized in the presence of inhibitors, cells were subjected to a heavy-isotope density shift in the presence or absence of the drugs. Before the addition of dense amino acids to intact monolayers (0 h), receptor was solubilized fromthe cells with Triton X-100, and the extractwassubjected to
14182
Divergent Catabolic Processing of Insulin and Insulin Receptor
isopycnic banding on cesium chloride gradients. As shown in Fig. lA, 1251-insulinbinding activity in the fractionated gradients exhibited a peak at fraction 25. When media containing dense (15N-,I3C-, and ’H-substituted) amino acids were added to thecells, the amplitude of the peak at fraction 25 decayed in a time-dependent manner, with a corresponding increase in binding activity centered at gradient fraction 16, the equilibrium position of newly synthesized “dense” receptor. As shown in Fig. lC, after 13 h of treatment with dense amino acids in theabsence of cycloheximide, the peak at fraction 25 had decayed to roughly half the peak height seen in panel A, with the generation of a peak of newly synthesized, dense 40 receptor at fraction 16. Thirteen hoursafter the simultaneous addition of dense amino acids and cycloheximideto themonolayers, no newly synthesized insulin binding activity could 20 be detected at or around fraction 16 (Fig. lB),indicating that CHX cycloheximide was inhibiting the synthesis of new receptor. Comparison of the panels of Fig. 1 also demonstrates that “ 0 cycloheximide completely prevented the inactivation of light 0 3 6 9 12 receptor. After 13 h of exposure to dense amino acids, the Hours “light” peak centered at fraction 25 in control cells (panel C) FIG.2. Inhibition of down-regulationby cycloheximide.At had decayed to about half the receptor level found before zero time, 1.7 p~ insulin ( I N S ) was added to confluent monolayers initiation of the density shift (panel A ) . Cycloheximide treat- to initiate down-regulation, and surface binding of 0.6 nM lBI-insulin ment completely blocked this decay of total receptor (panel to intactmonolayers a t 4 “Cwas assessed at timed intervals thereafter At time pointsindicated by the arrows, aliquots of cycloheximide B). Cycloheximide also blocked the insulin-induced receptor (0). (CHX) were added to the monolayers to a final cycloheximide condown-regulation process in these cells (Fig. 2). Cycloheximide centration of 20 pM, and surface binding was assessed at timed was added to the monolayers at 0, 2, 4, or 6 h after the intervals thereafter (X). Control cell monolayers had a specific cell addition of insulin, and cell surface binding was assessed at surface insulin binding capacity of 10 fmol. timed intervals thereafter. Addition of cycloheximide to the cells at any stage of the down-regulation time course led to the abrupt attenuationof the down-regulation process. From the data of Fig. 1 it appeared that the addition of cycloheximide resultsin a “freezing” of thetotal cellular receptor level. Fig. 2 indicates that thedrug inhibited perturbations of the plasma membrane receptor level. To examine the time course of this freezing process more systematically, surface andtotal cellular receptor levels were assayed in parallel, under four sets of conditions: in the presence of 1)
z
z
0
4
8
12, 0
4‘
8
12
TIME, hr. FIG.3. Time course of the effect of cycloheximide on surface and total cellular insulin receptor. Confluent monolayers were treated with 1.7 p~ insulin alone (0)or 20 PM cycloheximide alone (A), co-incubated with both 1.7 p~ insulin and 20 p~ cyclohexand synthesis. At zero time, dense amino acids, either in theabsence imide (O), or preincubated with 1.7 ~ L Minsulin for 2 h followed by or presence of 20 ~ L cycloheximide, M were added to confluent mono- treatment with both 1.7 p~ insulin and 20 p~ cycloheximide (m). At layers of 3T3-C2 cells, as described under “Materials and Methods.” timed intervals thereafter, monolayers were subjected to the ligand At 0, 3, 6, 9, 13, and 24 h after the addition of dense amino acids, debinding procedure and either assayed for cell surface insulin bindinsulin receptor was solubilized from the cell membranes, isopycni- ing capacity (panel A ) or detergent-solubilized and assayed for total cally banded in CsCI, and quantitated. 0, total insulin binding a t 0.6 cellular insulin binding capacity (panel B ) . Cell surface insulin bindnM 1251-insulin;X, nonspecific insulin binding at 0.6 nM 1z51-insulin ing capacity in control, untreated monolayers (the 100% level) is 10 and 3 ~ L Munlabeled insulin. Panel A, gradient profile of insulin fmol/6 cm of monolayer and 12 fmol/6 cm of solubilized monolayer. binding a t zero time; panel B , gradient profile of insulin binding 13 h after the addition of dense amino acids containing 20 PM cycloheximide (CHX);panel C, gradient profile of insulin binding 13 h after insulin alone to establish the down-regulation process, 2) the addition of cycloheximide-free dense amino acids. The uertical cycloheximide alone, 3) insulin and cycloheximide added sidashed lines indicate the peak positions to which “old‘ light receptor (fraction 25) and “new” heavy receptor (fractions 16-17) migrate. multaneously, and 4) cycloheximide and insulin after a 2-h Light receptor from control cells decayed in this experiment with a preincubation with insulin. The results of the experiment are shown in Fig. 3. Down-regulation proceeded normally at both half-life of 9 h. Fraction Number
FIG.1. Effect of cycloheximide on insulin receptor decay
Divergent Catabolic Processing of Insulin and Insulin the cell surface (Fig. 3A) and with total cellular receptor (Fig. 3B). However, no change in thereceptor level was seen either with cycloheximide present alone or when added simultaneously with insulin. The addition of cycloheximideto the cells 2 h after the addition of insulin resulted in therapid cessation of down-regulation, as manifest at both the cell surface and total cellular receptor. Cell viability was not affected by 20 *M cycloheximide until longer than 18 h after the initial exposure of the cells to thedrug. To verify that theeffect of cycloheximideon insulin receptor metabolism is due to the inhibition of protein synthesis and not some other effect of cycloheximide itself, two other inhibitors of protein synthesis, puromycin and pactamycin, were utilized. At 200 PM puromycin, protein synthesis was inhibited 98% and cell viability was maintained at control levels for >10 h. Both cell surface and total cellular insulin binding were assessed under conditions described above for cycloheximide. Whether puromycin was present alone or in combination with insulin, both cell surface and totalcellular receptor levels remained constant in thepresence of the drug (data notshown), consistent with the findings with cycloheximide. With 1~ L pactamycin, M protein synthesis was inhibited, but after 7 h, cell viability began to be reduced.Nevertheless, the substantial degree of insulin-induced receptor down-regulation at 6 h of both cell surface and totalreceptor level was totally blocked (data not shown) as had also been seen with both cycloheximide and puromycin. Thus,the immediate freezing of both cell surface and totalcellular receptor is due $0 the common effect of these drug? in inhibiting protein synthesis. Three steps in insulin receptor metabolism were investigated as potential sites at which the inhibition of protein synthesis could result in freezing of cellular receptor metabolism: 1)insertion of receptor into the plasma membrane, 2) internalization of receptor from the plasma membrane, and 3) intracellular inactivation of receptor to a form incapable of binding insulin. The rapid, insulin-induced translocation of insulin receptor from the cell surface to a trypsin-resistant compartment was utilized as an index of the ability of the cells to internalize receptor in thepresence of cycloheximide. When monolayers were incubated in the presence of cycloheximide for 1h and then exposed to both cycloheximide and insulin, cell surface insulin receptor rapidly translocated to an intracellular site in response to insulin addition, with kinetics identical to cycloheximide-free cells (Fig. 4, top). This indicates that cycloheximide does not affect the insulin receptor internalization process in these cells. Subsequent to the rapid (e30 min) insulin-induced internalization of receptor, a decay of internalized receptor binding activity was observed in cycloheximide-free cells which occurred much moreslowly (hours). This inactivation of internalized receptor was inhibited in cycloheximide-treated cells with a conservation of total cellular binding activity (Fig. 4, top). Actinomycin D at 0.8 PM levels had the same effect as cycloheximideon insulin-induced internalization and subsequent decay of receptor binding activity (Fig. 4, top). However, actinomycin D inhibited general protein synthesis.by less than 20%. It had been previously demonstrated (8) that while the addition of insulin causes the rapid internalization and redistribution of cell surface insulin receptor, this internalized receptor could be recycled back to the plasma membrane upon the removal of the extracellular insulin. This bulk recycling of internalized insulin receptor was utilized here to monitor the effect of cycloheximide on the insertion of internalized receptor into the plasma membrane. As demonstrated in Fig.
a
0
100
w
I’
14183
Receptor I
I
I
I
I
I
I
+Ins. +CHX. Total
0
80 -I
f-
60
E
a
6
I-
s
40
20
0
-d= a
0 9o
60-i
lii 9
E
I-w
5
Z 0 %
Conbol
3 i
0
+CHX
.
0-Q
t
K S
so si
-:(‘la . -
\P
2 0 -0
00
*
*
.
*
20 40 60 00 100 120 TIME, mb.
Effects of cycloheximide on insulin-induced receptor internalization and recycling. Top, the internalization of insulin receptor. Cell monolayers were preincubated with (0,0) or without (m,0 ) 200 p~ cycloheximide ( C H X ) or with 1 p~ actinomycin D (A) for 1 h before the addition of 1.7 p~ insulin (Ins.) at zero time. Total receptor (El, H) or internal receptor (0,0, A) was monitored at timed intervals thereafter, as described under “Materials and Methods.” Bottom, the recycling of internalized insulin receptor to thecell surface. Insulin (1.7 PM) was added at zero time t o induce the internalization of receptor. At 30 min, half of the monolayers received 200 p~ cycloheximide,and aftera 20-min incubation in the presence of both cycloheximide and insulin (0) or insulin alone (O), the monolayers were washed extensively to remove insulin (ligand debinding) while still in the presence (0) or absence (0)of 200 p~ cycloheximide. The levels of total, cell surface, and internal (resistant to trypsin) receptor were monitored at each point as described under “Materials and Methods.” FIG. 4.
4 (bottom),the addition of insulin to themonolayers resulted
in a rapid increase in the size of the intracellular receptor population, such that within 30 min after insulin addition, 50% of the total cellular receptor population resides in the intracellular compartment. Upon removalof the extracellular insulin, the level of intracellular receptor decays and ultimately returns to the time 0 receptor level. The totalcellular receptor level is constant over the time course of the experiment shown in Fig. 4 (bottom) (data not shown). Therefore, the decay in the internal receptor level demonstrated upon removal of insulin is due to the rapid re-insertion of receptor into the plasma membrane. As demonstrated in Fig. 4 (bottom), the re-insertion of insulin receptor into the plasma membrane was unaffected by cycloheximide. To further assess the effects of protein synthesis inhibitors
Divergent Catabolic Processing of Insulin and Insulin Receptor
14184
on the insertion of intracellular receptor into the plasma membrane, cell surface receptor was proteolytically inactivated, and thetime-dependent recovery of cell surface binding activity was determined in the absence or presence of cycloheximide or puromycin. Monolayers were proteolyzed under very mild conditions following a preincubation with cycloheximide (Fig. 5 B ) or puromycin (Fig. 5C). After removal of the trypsin, inhibitor-containing media were replaced and the recovery of cell surface insulin binding capacity was monitored a t intervals following proteolysis. The control monolayers regained insulin binding capacity in a linear manner (Fig. 5A). A full complement of receptor was attained 24-36 h after proteolysis (data notshown). Cell monolayers pretreated with cycloheximide (Fig. 5 B ) or puromycin (Fig. 5C) exhibited an initial rate of binding recovery similar to the control rate, indicating that insertion occurred normally in the inhibitortreated cells. After 6 h, however, the intracellular pool of receptor was depleted in these monolayers; thus, additional receptors could not be recruited to the cell surface. It is of interest that the cell surface receptor level in both the cycloheximide- and puromycin-treated monolayers declined after reaching peak levels of 15% recovery. Cell viability remained a t control levels throughout the timecourse of the experiment, so loss of cells from the monolayer did not account for the decline. Since inhibitor treatment caused the total receptor level to remain constant, it is evident that the decline in receptor level was due to internalization of the receptor. In spite of this later decline in receptor level, treatment of the monolayers with protein synthesis inhibitorsdoes not appear to affect the initial rates at which insulin receptor is inserted into the plasma membrane. It appears, therefore, that the inhibition of proteinsynthesis does not affect either the insertion of insulin receptor into theplasma membrane or its internalization from the plasma membrane. The locus of the effect appears to be at the level of receptor inactivation. Effects of Chloroquine on Insulin Receptor MetabolismThe effects of chloroquine on the insulin-induced rapid internalization and recycling of receptor were investigated. As observed with cycloheximide, preincubation of cell monolayers with 200 JCMchloroquine had no effect on therapid insulininduced internalization of the insulin receptor (Fig. 6A, 0-1 h). However, unlike the effects with cycloheximide, chloroquine had no effect on the subsequent inactivation of the
I
0
+CHX
+PUR0
3
m
t - 0
0
1 0
0
1
2 3 4 TIME. hr.
5
6
20 40 60 80 DO 1 2 0 TIME, mln.
TIME. mln.
0
20 40 60 80 100 120 TIME, mln.
FIG. 6. Effects of chloroquine on the insulin-induced receptor internalization and receptor recycling. Panel A, the internalization and inactivation of insulin receptor. Cell monolayers were or without (0)200 p~ chloroquine preincubated for 20 min with (0) (CQ) before the addition of 1.7 PM insulin (INS). The level of intracellular receptor was monitored as decribed under “Materials and Methods.” Panel B, the effect of chloroquine on insulin receptor recycling: chloroquine addition following insulin addition. Following a 30-min preincubation with 1.7 p~ insulin, cells were subjected to an additional 20-min incubation in the absence (0)or presence (0) of 200p~ chloroquine. Insulin was then removed from the cell culture of chloroquine. The level of media in the absence ( 0 )or presence (0) internal insulin receptor was quantitated as described under “Materials and Methods.” Panel C, the effect of chloroquine on the recycling of internalized insulin receptor to the cell surface: chloroquine addition preceding insulin addition. Confluent cell monolayers were preor without (0)200 p~ chloroquine for 20 min before treated with (0) the addition of 1.7 pM insulin. After a 30-min incubation with insulin, the hormone was removed from the monolayers in the absence (0) or presence (0)of chloroquine. Internal insulin receptor levels were determined as described under “Materials and Methods.” Panel D, the effect of chloroquine on insulin receptor recycling: the simultaneous addition of chloroquine and insulin. Either 1.7 ~ L insulin M alone (0)or insulin and chloroquine together (0) were added to confluent monolayers. After a 30-min incubation, insulin was removedfrom the cell culture media while maintaining the absence (0)or presence (0) of chloroquine. The intracellular receptor level was monitored as described under “Materials and Methods.”
internalized receptor (Fig. 6A, 1-6 h). Chloroquine did, however, affect the re-insertion of internalized receptor into the plasma membrane. When monolayHours ers were subjected to chloroquine treatment after the insulinFIG. 5. Recovery of cell surface insulin binding capacity induced rapid internalization of receptor, subsequent removal after trypsin treatment in the presence of cycloheximide or of insulin resulted in theinsertion of receptor into theplasma puromycin. Confluent monolayers were pretreated with either 20 membrane at a rate similar to the control rate (Fig. 6 B ) . If, ~ L cycloheximide, M or 200 p~ puromycin for 1.5 h before being washed once with 4 ml of serum-free media and proteolyzed with trypsin (20 however, cell monolayers were incubated with chloroquine pg/ml of PBS) for 20 min a t 37 “C. The trypsin-containing buffer before the addition of insulin, recycling of internalized recepcell surface was not only inhibited, buta significant was aspirated from the monolayers a t zero time and replaced with tor to the complete media containing soybean trypsin inhibitor(60 pg/ml). This additional increase in thesize of the internalpool of receptor medium was removed and replaced with complete media without was detected (Fig. 6C). Concomitant addition of insulin and inhibitor (panel A ) , with 20 p~ cycloheximide ( C H X ) (panel B ) , or chloroquine produced intermediate results(Fig. 6D): re-inserwith 200 JIM puromycin (PURO) (panel C), and themonolayers were returned to the incubator. Cell surface insulin binding capacity was tion of receptor into the plasma membrane was not totally then determined at thetimes indicatedas described under “Materials inhibited, but was considerably slowed compared to control (chloroquine-free) cells. Over the time course of the experiand Methods.”
Divergent Catabolic Processing of Insulin and Insulin Receptor ments shown in Fig. 6, B-D, no change in the total receptor level was observed. These data indicate that chloroquine does not affect insulin receptor internalization or inactivation, but inhibits the reversal of the insulin-induced internalization process, depending on the order of addition of insulin and chloroquine. Effects of Cycloheximide and Chloroquine on Insulin Degradation-The time course of degradation of insulin by 3T3C2 fibroblasts is shown in Fig. 7. After a 10-15-min lag, the rate of insulin degradation is linear over the 2-h time course. The ratesof insulin degradation under the multiple treatment conditions described in thelegend to Fig. 3 are shown in Table I. Chronic treatment of the cells with cycloheximide at levels that totally inhibit receptor inactivation (Fig. 4, top) did not impair the rate of insulin degradation whencompared to control degradation rates. However, chronic treatment of cells with insulin, which ledto a decrease in thelevel of cell surface insulin receptor, also led to a substantial decrease in the rate of insulin degradation. A comparison of the rates of insulin degradation and the level of cellsurface insulin binding is illustrated in Fig. 8. The data for cell surface insulin binding is from Fig. 3A, where the 100% level is equivalent to 10 fmol of specifically bound
I
I
I
14185 I
I
I
r = 0.997 slope =0.95 t
”
3 20 ln t
H
0
40 60 80 100 ‘251-1nsulin Bound, %Control
0
20
FIG.8. Correlation of insulin degradation with cell surface insulin binding.Insulin degradation data were taken from Table I, with the symbols corresponding to the various cycloheximide and insulin treatments described in the legend to Fig. 3. The 100% level of the rate of insulin degradation is equivalent to 6.1 fmol/h/l.6 X lo6cells. Cellsurface insulin bindingdata arefrom Fig. 3. The 100% level of insulin binding is 10 fmol/l.6 X lo6 cells. The least square fit line drawn through the datapoints has a slope of 0.95-and a correlation coefficient of 0.997.
v ) ”0
20 40 60 80 100 120 TIME, min.
FIG. 7. Time course of insulin degradation. Cell monolayers were subjected to the ligand debinding procedure with serum-free media containing 1%bovine serum albumin. 1251-Insulindegradation was then initiated and quantitated as described under “Materialsand Methods.” The data arepresented as femtomoles of insulin degraded per 1.6 X lo6 cells.
TABLE I Insulin degradatwn in cycloheximide-or insulin-treated cells Monolayers were treated with cycloheximide and insulin in the combinations described in the legend to Fig. 3 for 12 h. All of the monolayers were then subjected to the ligand debinding procedure with serum-free media containing 1%bovine serum albumin. Monolayers that had been pretreated with cycloheximide were also “debound” with cycloheximide-containing media. Following ”debinding,” ‘251-insulindegradation was initiated and quantitiated as described under “Materials and Methods.” Treatment
Insulin degradation
fmol/h/l.d X
IO6 cells
None 6.1 2.2 +Insulin +Cycloheximide 6.4 +Cycloheximide + insulin (simulta6.1 neous addition) +Insulin + cycloheximide”(insulin 4.0 preincubation) Monolayers were treated with insulin for 2 h before the addition of cycloheximide.
1251-insulin,and insulin degradation rates are from the data of Table I, where the 100% level is 6.1 fmol/h. The plot in Fig. E) shows a linear one-to-one relationship between insulin receptor level and insulin degradation. This correlation indicates that insulin degradation is receptor-mediated. The dependence upon insulin concentration of the rate of insulin degradation in theabsence or presence of prior chronic (12 h) cycloheximide treatment is shown in Fig. 9. The rate of insulin degradation appears to be a linear function of insulin concentration up to insulin concentrations of 10-12 nM. Above 12 nM insulin, departure from linearity is apparent. Cycloheximide had no effect on the magnitude or shape of the insulin degradation dose-response curve. The effect of chloroquine on the rate of accumulation of cell-associated ‘‘’1 label and the degradation of insulin to trichloroacetic acid-soluble form in cells incubated with lz5Iinsulin is shown in Fig. 10. Upon addition of ‘l-insulin to cell monolayers either in the presence or absence of chloroquine, cell-associated 1251activity rapidly increased, overshot to a small but reproducible degree, and then plateaued at a steady state level. In the presence of chloroquine, the steady state level of cell-associated radiolabel was approximately 60% higher than in the control cells (Fig. 1OA). The production of trichloroacetic acid-soluble radiolabel in the medium (“insulin degradation”) commenced 10-15 min after the addition of ‘251-insulinto the monolayers, as also shown in Fig. 7. In the presence of chloroquine, the rate of insulin degradation was inhibited by approximately 70% (Fig. 1OB) with no apparent change in thelevel of cell surface insulin receptor. These results indicate that cycloheximide,at concentrations which inhibit insulin receptor inactivation, has no effect on the rate of insulin degradation. Chloroquine, however, which
14186
Divergent Catabolic Processing of Insulin and Insulin Receptor
increased receptor inactivation with no change in receptor synthetic rates (1, 2). The question was raised, how could cycloheximide,an inhibitor of protein synthesis, inhibit downregulation when down-regulation itself did not perturb the E20 synthetic rate? It was found in density shift experiments (Fig. O \ 1)that cycloheximide not only completely inhibited insulin 0 receptor synthesis, but completely suppressedthe inactivation I6 of the receptor (Fig. 1B). Puromycin and pactamycin, other inhibitors of protein synthesis with different mechanisms of d action from cycloheximide(14),also caused the same freezing of receptor level. This indicated that the process was due to x12 the general inhibition of protein synthesis and was not an E effect specificto any one of the inhibitors. (3 To identify the locus of cycloheximide action, a number of cellular processes were monitored internalization of the receptor from the plasma membrane, recycling of internalized receptor, and insertion of the receptor into the plasma membrane. Insulin can induce the rapid translocation of insulin $ 4 receptor from the cell surface to anintracellular site ineither z_ the presence or absence of cycloheximide (Fig. 4, top). The recycling of receptor also appears to be unaffected by inhibition of protein synthesis (Fig. 4, bottom), as is the insertion 0 of receptor into theplasma membrane (Fig. 5). The reappear0 4 8 12 16 20 ance of cell surface specific insulin binding capacity after mild ClNSULlN3, nM proteolysis indicated that approximately 3-5% of the normal FIG. 9. Insulin degradationas a function of insulin concen- cellular complement of receptor is inserted into the plasma tration in cycloheximide-treated or -untreatedcells. Half of membrane every hour. Approximately the same initial rates the cell monolayers were treated with 20 &M cycloheximide for 12 h of insertion were observedin cycloheximide- and puromycinbefore the addition of '251-insulin. Insulin degradation was initiated treated cells (Fig. 5). However, since the synthesis ofnew by replacing the old media with fresh pre-equilibrated media containing '9-insulin at the desired concentration in the presence (0)or receptor was inhibited, the small intracellular pool of receptor absence (0)of cycloheximide. Time points a t 20 and 60 min were was soon depleted and the rates of insertion onto the cell utilized to determine the rate of insulin degradation a t each insulin surface plateaued (Fig. 5, B and C). It is of interest that at concentration. later times, the inhibitor-treated cell surface receptor level declined. Since cellviability was not affected at the time points at which the decline was observed, the surface receptor may be internalizing to produce a new steady state distribution of cellsurface and intracellular receptors.Following 12 CHLOROQUINE proteolysis, no initial "burst" of cell surface binding activity was detected in this cell line as was reported for 3T3-Ll adipocytes (15). 0-d While insulin-induced translocation of receptor from the 85 a cell surface to an intracellular site is not affected by protein a m synthesis inhibitors, the subsequent decay of binding activity W -I 0 J in theintracellular compartment, observed in cycloheximidew /* u free cells, is totally inhibited in thepresence of cycloheximide (Fig. 4, top). It appears thatthe cycloheximide-inhibited TIME, min. factor required for the metabolic inactivation of the insulin FIG. 10. Effect of chloroquine on insulin binding and degradation. '251-Insulin (0.6 nM) was added to confluent monolayers receptor is notinvolved either in theinsertion of the receptor in the presence (0)or absence (m) of 200 FM chloroquine in Krebs- into theplasma membrane or the internalization of the recepRinger phosphate buffer containing 1%bovine serum albumin. At tor to an intracellular compartment. It is possible, however, various time points, the buffer was aspirated and precipitated with that thefactor, perturbed by the cessation of protein synthetrichloroacetic acid for evaluation of insulin degradation (panel B ) , sis, acts directly on the receptor molecule to inactivate or and the monolayer was quickly washed with cold PBS for determination of cell-associated '2514nsulin (panel A ) , as described under mark it for inactivation. Others have suggested the requirement of a product of protein synthesis to maintain protein "Materials and Methods." breakdown (16-19). These earlier studies, performed either in cell culture (17) or with perfused organs (18, 19), indicated inhibits insulin degradation, does not affect insulin receptor that general protein degradation was inhibited within 30 min internalization and inactivation. after the addition of inhibitor and suggested that theinhibition of protein breakdown was not due to an accumulation of DISCUSSION precursors of protein synthesis (17). In thepresent study, the The inhibition of the insulin-induceddown-regulation proc- inhibition of protein synthesis might be expected to lead to ess by cycloheximide has been reported in a number of cell larger pools of precursors used in protein synthesis which types ( 3 4 , in addition to the present study (Fig. 2). The might act to stabilize the insulin receptor population. Actiunusual nature of this effect of cycloheximide on receptor nomycin D, which blocks RNAsynthesis but did not materidown-regulation was noted using the heavy-isotope density ally affect protein synthesis, also inhibited the inactivation of shift technique which showed that down-regulation caused the insulin receptor (Fig. 4, top). It is not likely, therefore, I
-
a
28
z
Divergent Catabolic Processing of Insulin and Insulin Receptor that in the presence of cycloheximide, the insulin receptor population is beingstabilized by precursors of protein synthesis. Our results with cycloheximide suggest, therefore, that receptor inactivation occurs through the action of a shortlived protein. Moreover, the results with actinomycin D suggest that the messenger RNA for this protein turns over rapidly in 3T3-C2 cells. While cycloheximideinhibits receptor inactivation, chronic treatment of the cells withthe agent has no effecton insulin degradation (Table I). Insulin degradation in these cells appears to be receptor-mediated,as evidenced bythe correlation between the cell surface receptor level and the insulin degradation rate (Fig. 8). It appears, therefore, that .in the presence of cycloheximide,the insulin-receptorcomplex is internalized, and the ligand is discharged from the receptor and targeted for degradation as in untreated cells. Since inactivation of receptor does not occur in thepresence of cycloheximide, the ligand and the receptor must separate at some subcellular location following internalization, but preceding delivery to the lysosomal compartment. Chloroquine, on the other hand, has no effect on the rapid insulin-inducedtranslocation of receptor oron its subsequent inactivation (Fig. 6A), but decreases the rate of insulin degradation (Fig. 10). In addition to these findings in fibroblasts, in an hepatocyte culture system, chloroquine was found to have no effect on the insulin receptor turnover (11).The use of this second inhibitor provides corroborative evidence that receptor inactivation is a process that occurs independently of insulin degradation. By electron microscopy, a number of investigators have shown that in the presence of chloroquine, ‘9-labeled insulin or ferritin-labeled insulin becomes localized in intracellular structures (20, 21). The mechanism by which chloroquine is believed to act is through its scavenging the protons within endosomes or lysosomes, causing an increase in the pH of these organelles (22,23). Within the lysosomes,this increased pH impairs the activity of lysosomal hydrolases, depressing the degradation of insulin and causing intact insulin to build up within these organelles. This model is consistent with electron microscopic studies (20) and the findings shown in Fig. 10 demonstrating decreased insulin degradation and increased cell-associated 1251-insulin-derived radiolabel in the presence of chloroquine. There is mounting evidence that acidification is an important process in endocytic vesicles which promotes the discharge of ligand from receptor (for review, see Ref. 24). Thus, in the present study, chloroquine may not only beacting at thelevel of lysosomes, but may also be preventing the acidification of endocyticvesicles. The inhibition of ligand discharge from receptor at thelevel of the endocytic vesicleis likely to be the reason for the chloroquineinduced inhibition of recycling demonstrated in Fig. 6, C and D. Therefore, in order to inhibit recycling of the insulin receptor, chloroquine must be added to thecells before orat the same time that insulin is added to induce internalization (Fig.6). A similar dependenceon the order and time of addition of chloroquine has also been describedin studies of Semliki Forest virus absorption and infection of baby hamster kidney cells (25). This finding suggests that the acidification process occurs very quickly after internalization, such that the internalization of insulin-receptor complexes and chloroquine together is required to prevent the acidification-dependent discharge. The presence of chloroquine didnot, however, affect the rate of inactivation of internalized receptor (Fig. 6A), suggesting that the receptor molecule is modified to lose binding activity via an acid-independent process ( i e . at a nonlysosomal site).
14187 *A A A
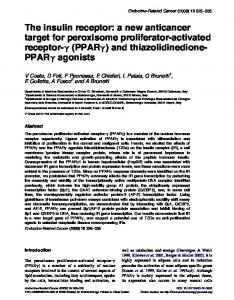
* Lysosome FIG. 11. Proposed model for the divergent catabolic processing of insulin and the insulin receptor. Refer to text for details.
These results obtained through the use of cycloheximide and chloroquine lead to the model schematized in Fig. 11. Upon binding to insulin, cell surface receptors are rapidly internalized (Step 1 ). The compartment containing the internal ligand-receptor complexesis acidified possibly through a proton pump as demonstrated in coated vesicles (26), leading to the discharge of ligand from the receptor (Step 2 ) . Once ligand is discharged, the receptor is free to recycle backto the plasma membrane(Steps 3 and 4 ) . Discharge of ligand seems to be required for recycling sincereceptor, chemically crosslinked to insulin, will readily internalize but not reappear on the cell surface? Chloroquine may act to inhibit this acidification process by preventing the separation of ligand from receptor (Step 2 ) , leading to the inhibition of recycling. Inactivation of the insulin receptor ( i e . loss of binding activity) appears to occur at anintracellular site (Steps 5 and 6)via a cycloheximide- and actinomycin D-sensitive process. Since thisstep is not chloroquine-sensitive, it is reasonable to conclude that theinactivation 1) is not acidification-dependent and 2) can be performed on intact ligand-receptor complexes (Step 6 ) as well as on ligand-free receptor (Step 5). Further evidence that ligand-receptor complexes can be inactivated and degraded comes from investigations with photoaffinity-labeled, cross-linked receptor(10, 27). Insulin degradation (Step 7) has been shownto be a chloroquine-sensitive process, with the chloroquine locusof action frequently cited to be at thelysosome. However, if chloroquine’sinitial site of action is at the endocytic vesicle,preventing acidification and the suisequent discharge of insulin from the receptor, the results seen in Fig. 10 would be expected a build-up in cellassociated radioactivityand a decrease in insulin degradation. The degradation of the inactive insulin receptor may also occur in the lysosome (Steps 8 and 9 ) ,but methods other than binding assays will be requiredto investigate this process. Acknowledgments-We would like to thank Norma Mitchell and Deborah Lee for expert secretarial assistance. REFERENCES 1. Knutson, V. P., Ronnett, G. V., and Lane, M.D. (1982) Proc.
Natl. Acad. Sci. U. S. A. 79,2822-2826 2. Ronnett, G . V., Knutson, V. P., and Lane, M. D. (1982) J. Biol. Chem. 257,4285-4291 3. Peterson, B., Beckner, S., and Blecher, M. (1978) Bwchim. Biophys. Acta 542,470-485 4. Reed, B. C., Ronnett, G. V., and Lane, M. D. (1981) Proc. Nutl. Acad. Sci. U.S. A. 78,2908-2912
V. P. Knutson and M. D. Lane, unpublished observations.
14188
Divergent Catabolic Processing of Insulin and Insulin Receptor
5. Kosmakos, F. C., and Roth, J. (1980) J. Bid. Chem. 255, 9860-
9869 6. Hinkle, P. M., and Tashjian, A. H., Jr. (1975) Biochemistry 14, 3845-3851 7. Saez, J. M., Haour, F., Tell, G. P. E., Gallet, D., and Sanchez, P. (1978) Mol. Phrmacol. 14,1054-1062 8. Knutson, V. P., Ronnett, G. V., and Lane, M.D. (1983) J. Bid. Chem. 258,12139-12142 9. Hammons, G. T., and Jarett, L. (1980) Diabetes 29,475-486 10. Heidenreich, K. A., Brandenburg, D., Berhanu, P., and Olefsky, J. M. (1984) J. Biol. Chem. 259,6511-6515 11. Krupp, M. N., and Lane, M. D. (1982) J. Bwl. Chem. 257,13721377 12. Gavin, J. R., Roth, J., Neville, D. M., DeMeyts, P., and Buell, D. N. (1974) Proc. Natl. Acad. Sci. U. S. A. 71,8688 and Livingston, J. N. (1978) Proc. Natl. Acad. Sci. 13. Krupp, M. N., U. S. A. 75,2593-2598 14. Pestka, S. (1971) Annu. Reu. Microbwl. 25,487-562 15. Deutsch, P. J., Rose, 0. M., and Rubin, C. S. (1982) J. Bid. Chem. 257,5350-5358
16. Hershko, A., and Tomkins, G. M. (1971) J. Bwl. Chem. 246, 710-714 17. Epstein, D., Elias-Bishko, S., and Hershko, A. (1975) Biochemistry 14,5199-5204 18. Rannels, D. E., Kao, R., and Morgan, H. E. (1975) J. Bwl. Chem. 250,1694-1701 19. Woodside, K. H. (1976) Biochim. Biophys. Acta 421,70-79 20. Smith, R. M., and Jarett,L. (1982) Proc. Natl. Acad. Sci. U. S. A. 79,7302-7306 21. Carpentier, J.-L., Gorden, P., Freychet, P., Le Cam, A., and Orci, L. (1979) J. Clin. Inuest. 63, 1249-1261 22. DeDuve, C, DeBarsy, T., Poole, B., Trouet, A., Tulkens, P., and Van Hoof, F. (1974) Biochem. Pharmaeol. 23,2495-2531 23. Ohkuma. S.. and Poole. B. (1978) Proc. Natl. Acad. Sci. U. S. A. 75,3327-3331 24. Steinman. R. M.. Mellman, I. S., Muller, W. A., and Cohn, Z. A. (1983) j . Cell hiol. 96,l-27 25. Helenius, A., Marsh, M., and White, J. (1982) J. Gen. Virol. 58, 47-61 26. Stone, D. K., Xie, X.-S., and Racker, E. (1983) J. Bid. Chem. 258,4059-4062 27. Reed, B. C. (1983) J. Bwl. Chem. 258,4424-4433 I
.
.