A pop-up window listing the top 10 users and their scores was ... subjects' satisfaction toward the computer-simulated training program. The two instruments are.
+XQJ��3��3���06F�51���&KRL��.��6���3K'���&KLDQJ��9��&��/���3K'�51������ ��3UH�SULQW�YHUVLRQ &RUUHVSRQGHQFH�DXWKRU���&KRL��.��6���6FKRRO�RI�1XUVLQJ��7KH�+RQJ�.RQJ�3RO\WHFKQLF�8QLYHUVLW\��+XQJ�+RP��.RZORRQ��+RQJ�.RQJ 7HO���������������������(PDLO���WKRPDVNV�FKRL#SRO\X�HGX�KN��� 7KLV�ZRUN�ZDV�VXSSRUWHG�LQ�SDUW�E\�WKH�+RQJ�.RQJ�5HVHDUFK�*UDQWV�&RXQFLO��3RO\8��������(
Using interactive computer simulation for teaching the proper use of personal protective equipment
Abstract The use of personal protective equipment (PPE) is one of the basic infection control precautions in health care. The effectiveness of PPE is highly dependent on adequate staff training. In this paper, a computer simulation program, as a supplement to conventional training approaches, was developed to facilitate the learning of the proper use of PPE. The simulation program was a webbased interactive software with user-friendly graphical interface for users to practise the use of PPE usage via drag-and-drop metaphors and respond to questions online. The effectiveness of the computer simulation software was investigated by a controlled study. Fifty healthcare workers were randomly assigned into 2 groups: one received conventional PPE training only (control group), the other also received the same conventional training but followed by using the developed simulation program for self-learning (experimental group). Their performance was assessed by PPE donning and doffing evaluation before and after the training. The results showed that the computer simulation program is able to improve the healthcare workers’ understanding and competence in using PPE.
Keywords: Personal protective equipment; computer-simulated training; online learning; nursing education.
Background The outbreak of severe acute respiratory syndrome (SARS) in 2003 affected thousands of healthcare workers worldwide. As a lesson learnt from the epidemic, infection control and occupational health became an area of focus to safeguard healthcare workers from infection hazards at work. The use of personal protective equipment (PPE) is an important approach to protect healthcare workers from acquiring occupational infections in healthcare settings. Examples of PPE include fit-tested N95 respirators, goggles or face shields, disposable longsleeved gowns and disposable gloves. However, improper use of PPE may instead lead to the spread of infectious agents among healthcare workers and patients. Although guidelines on the use of PPE have been developed, continuous outbreak of ward-related infections suggests the need to enhance the training of PPE usage for clinical staff. Many studies have demonstrated the effectiveness of different types of PPE in healthcare settings and their benefits for both healthcare workers and patients.1,2 However, it has also been shown that healthcare workers encounter difficulties of different extents in complying with the guidelines of PPE usage, where the lack of knowledge is one of the key determinants. Reid et al. examined the knowledge, self-reported behaviors and the barriers regarding the use of PPE of the employees in a pediatric department.3 The study found that 66% of the employees were deficient in the knowledge of proper PPE usage, which was considered as a major reason for low compliance with the guidelines. Similar findings were also obtained from a study by Sax et al. 4 As a result, even though PPE is used, lack of knowledge in donning and doffing may negate its intended effects and instead increase the risk of infections. For example, contamination can easily occur during the process of glove removal if the required procedures are not followed correctly. It is therefore necessary to educate healthcare workers about the correct use of PPE and increase
their competence. While many studies have also raised the importance of infection control training, particularly after the SARS outbreak 5, relatively few studies addressed the training methods and the efficiency. PPE training is conventionally conducted by education programmes through lectures, demonstrations and hands-on practice, with the aid of videos and printed materials.6 Recent decades have witnessed the increasingly important role of computer simulation in training and education. It has been considered as an effective and flexible way for healthcare training in a variety of situations. A main advantage of computer simulation is its ability to provide real-world experience with high level of realism and interactions,7 which enable experiential and active learning in virtual environments. A number of positive outcomes in training and learning with computer simulation have been reported, in terms of learner satisfaction, realism, value and knowledge. 8 Computer simulation is also a commonly adopted training approach for the management of healthcare institutions, attributed to the realistic scenarios simulated with computers.9 Despite the benefits and popularity of computer simulation in healthcare education, few studies address the use of computer simulation in infection control training, particularly the use of PPE. In this study, a computer-based training program was designed in attempt to complement conventional PPE training approaches and to enhance the donning and doffing skills of the healthcare workers. The effectiveness of the computer program was evaluated by assessing healthcare workers’ compliance with the donning and doffing procedure before and after using the computerized method for training. The details will be discussed in the following sections.
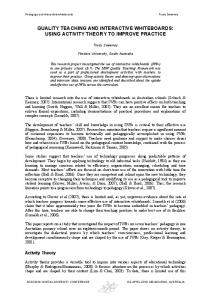
Methods The Computer Simulation Program In this study, a computer simulation program for PPE training was designed based on the infection control guidelines of the World Health Organization10 and the local infection control authority.11 The design of the simulation program put emphasis on the essential techniques and the required sequence of wearing and removing PPE. It simulated PPE donning and doffing procedures for precautions against airborne danger, where five types of PPE, including N95 respirator, face-shield, cap, gown and gloves, were required. The simulation program began by testing users about the donning procedures, where a virtual changing room with a healthcare worker preparing to put on PPE was shown on the screen (see Figure 1(a)). The five types of PPE were represented with the corresponding icons displayed at the bottom of the screen. The PPE could be dragged by the user with a computer mouse into the changing room, and put onto appropriate body parts of the virtual healthcare worker to signify the donning of a PPE. The user was required to put on the five types of PPE following the correct sequence. Animation of the donning procedure was played when the correct choice of PPE was made. After virtual donning of a PPE was made, the user was presented with multiple choice questions (with animated insets for each choice as shown in Figure 1(b)) about the use of that PPE in order to test the understanding about the correct donning steps. Visual prompts were invoked if a PPE was selected in the wrong sequence or the PPE was put on wrong body parts. The user could retry, request for a hint, or give up and ask for the correct answer (Figure 1(c)). The computer simulation program repeated the above procedure for each of the 5 types of PPE until they were all put on the virtual healthcare worker. The simulation was then followed by the doffing procedure.
Similar to the donning procedure, the correct sequence of removing the PPE put on the virtual healthcare works was tested. The user was required to click on a PPE to signify the removal of that PPE. For example, Figure 1(d) illustrates the removal of the glove. When an incorrect choice was made, a visual prompt was invoked where the user can retry, get a hint or give up. The user was then challenged by multiple choice questions concerning the proper way of removing that PPE (Figure 1(e)), followed by the playing of animations of the removal procedure. At this point, the user was also required to dispose the removed PPE to the appropriate trash bin, i.e. the one with lid on the right in Figure 1(f), by dragging the PPE icon with the computer mouse. The computer program further required the user to demonstrate the understanding of the need to wash hands after disposing each PPE, schematically by clicking on the virtual water sink with the mouse. These two steps – PPE disposal and handwashing – had to be carried out after the removal of each PPE. Failure would trigger visual prompts and the user must retry until the two steps were correctly completed. The computer-simulated training can be completed in around 10 to 15 minutes. User performance was recorded in terms of the completion time, the number of errors made, the number of hints requested, and the score. A point deduction policy was adopted in the computer program, where the maximum score of the training was 100 points; 5 points were deducted for every error made (e.g., picking a PPE in wrong sequence, selecting wrong answer for a multiple choice question, disposing PPE into wrong trash bin, or forgetting to wash hands); 2 points are deducted each time when a hint was requested. That means a user making excessive errors may have already got zero point before the end of the training. A pop-up window listing the top 10 users and their scores was shown on the screen at the end of the simulated training. The computer simulation program was a web-based application which was assessable online with a generic web
browser. The web server was able to log the activities of the users and collect user performance data.
Sampling As healthcare workers in out-patient clinic are at risk of contracting infectious diseases, the 24-hour out-patient department (OPD) of a private hospital was invited to participate in the study. The OPD is at the frontline of the hospital, responsible for triaging patients and handling different infectious patients before admission. Information about the study and consent forms were sent to all healthcare workers of the OPD, including registered nurses, enrolled nurses and healthcare assistants. Those who agreed to participate in the study, able to read English, and with basic computer operation skills, were recruited as subjects. The study was approved by the Human Subjects Ethics Committee of the institutional review board.
Instruments Two instruments were employed in the study, including the PPE donning and doffing evaluation form for measuring the subjects’ performance in actual gown-up and de-gown procedure; and the IBM Computer System Usability Questionnaire (CSUQ) for evaluating subjects’ satisfaction toward the computer-simulated training program. The two instruments are further described as follows. The PPE donning and doffing evaluation form has been and is currently used in the participating hospital to assess healthcare workers’ gown-up and de-gown skills. It was adopted in the study to evaluate the hands-on skills of the subjects. The evaluation form consisted of two parts, concerning the donning and doffing procedures respectively. It was a checklist designed for
assessor to record whether the healthcare workers had carried out the required steps and used the PPE properly during the process of donning and doffing. For example, during the donning process, the evaluation form checked if the healthcare worker had ensured a PPE was intact and well-fitted; confirmed the N95 respirator was properly secured around the face and performed seal check; or whether the worker had fastened the strings of PPE in correct sequence. In the doffing process, the form checked if the removed PPE was kept inside out; whether the strings of PPE were loosen in correct sequence, or whether the healthcare worker had disposed the removed PPE into a proper trash bin and performed handwashing. One point was given for an item in the form if the corresponding step was carried out correctly. Conversely, no point was given if the required step was missed or not performed correctly. In the participating hospital, the donning and doffing performance of healthcare workers is considered satisfactory if they can correctly perform at least 90% of the steps specified in the items of the evaluation form. For the purpose of the study, the content validity of the PPE donning and doffing evaluation form adopted was reviewed by a panel of three experts on infection control. They were respectively an academic specialized in occupational health, a senior nursing officer and a deputy in charge of an infection control department. The panel members assessed the content validity by rating the level of relevance of each item in the form using a 5-point Likert scale, from 1 (very irrelevant) to 5 (very relevant). They also provided comments on the items. After the review, one item was discarded from the original PPE donning evaluation from since it was considered repetitive by the panel, whereas the items in the doffing evaluation form were all rated ‘very relevant’ and thus kept for the study. Accordingly, the final version of the evaluation form used in the study contained 16 items for the donning and 20 items for the doffing section, and thus the corresponding total score of the two sections was 16 and 20 points. The content validity index
(CVI) of the donning and doffing sections was 0.94 and 1.0 respectively, showing that the evaluation form possesses good content validity12. The IBM Computer System Usability Questionnaire (CSUQ)13 is a psychometric instrument designed to collect subjective opinions and user satisfaction toward a computer system. It contains 19 items and adopts a 7-point Likert scale for each item, with 1 indicating ‘strongly agree’ and 7 indicating ‘strongly disagree’. The items concerns about general usability of computer system from several aspects, including ease of use, effectiveness, efficiency, productivity, information presentation and organization, interface, expectation on the functions and capabilities, and overall satisfaction with the system. The questionnaire has strong evidence of reliability. In the study, the CSUQ was adopted to evaluate the subjects’ overall satisfaction of the computer simulation program.
Research Design and Procedure An experimental study was conducted to evaluate the effectiveness of the proposed computer simulation program. The subjects were divided into two groups, one receiving conventional PPE training (control group), and the other receiving conventional PPE training plus computer-simulated training using the proposed simulation program (experimental group). The subjects were randomly assigned to the control and experimental group of the same size. A prepost test design was adopted to study the effectiveness of the two training approaches by using the PPE donning and doffing evaluation form to measure the subjects’ performance before and after the training. A survey administered by using the IBM CSUQ was conducted to evaluate user satisfaction toward the computer simulation program.
The research procedure is shown in Figure 2. It began with the pre-test where the two groups of subjects were required to perform the gown-up and de-gown procedures. Their performance was assessed using the PPE donning and doffing evaluation form by an infection link nurse of the participating hospital who was blinded about the research. Next, the subjects of both the control and experimental group attended conventional PPE training. In the training, they received a 15-minutes demonstration of PPE donning and doffing procedures by another infection control link nurse. After a week, the subjects of the control group were required to perform PPE donning and doffing again. Their performance was assessed with the evaluation form to yield the post-test results. For the experimental group, the subjects were asked to use the proposed computer simulation program to learn PPE donning and doffing. To reduce researcher bias, three research assistants were first trained to operate the computer simulation program and then responsible for teaching the subjects in the experimental group about the use of the simulation program. The subjects were expected to complete computer-simulated training within 15 minutes. After another week, the subjects in the experimental group were required to perform PPE donning and doffing, and their performance was assessed to obtain the post-test results. Furthermore, they were also asked to complete in the IBM CSUQ to collect their subjective opinion toward the simulation program.
Results Demographic Data Fifty healthcare workers took part in the study. Eighteen subjects (36%) aged between 20 and 30 years, 18 (36%) aged between 31 and 40 years, and 14 (28%) aged between 41 and 50 years. In terms of job ranks, 12 (24%) subjects were registered nurses, 10 (20%) subjects were
enrolled nurses and 28 (56%) subjects were healthcare assistants. Regarding their working experience in nursing, 15 (30%) subjects had 0 to 3 years of experience, 8 (16%) subjects had 4 to 6 years of experience, one (2%) subject had 7 to 9 years of experience and 26 (52%) subjects had more than 9 years of experience. The subjects were randomly assigned into the control group and the experimental group, each with a size of 25. Demographic data of the two groups are shown in Table 1. Statistical results indicated that there was no significant difference in age, (2 = 2.03, p = 0.36), rank (2 = 0.00, p = 1.00) and experience (2 = 0.08, p = 0.78) between the control and experimental groups. PPE Donning and Doffing Evaluation The performance of the subjects in PPE donning and doffing is shown in Table 2. As indicated in the last column of the table, Mann-Whitney U-test showed that in the pre-test, there was no significantly difference between the two groups for the donning (p = 0.859) and doffing evaluation (p = 0.055), whereas the post-test score of the experimental group was significantly higher than the control group for both the donning and doffing evaluation, with p = .013 and p < 0.000 respectively. On the other hand, Wilcoxon signed rank test showed that improvement in donning and doffing performance as observed in the post-test within each group was statistically significant. For the control group, the donning score and doffing score increased by 0.96 (p < .001) and 1.04 (p = .003) respectively. For the experimental group, the scores increased by 1.56 (p < 0.000) and 1.72 (p < 0.000) respectively. Correlation analysis was conducted to study whether the pre-test donning and doffing scores of all the subjects were related to the age, rank and working experience of the subjects. Refer to Table 3, analysis by Spearman’s rho showed no association between the pre-test scores and the
three demographic variables. The same analysis was also conducted for the post-test scores of the control and experimental group respectively. The results in Table 4 indicate that the post-test score of the control group was significantly associated with the age and rank of the healthcare workers, while the score of the experimental group showed no association with the three demographic variables. Errors in Simulated Training For the subjects in the experimental group, the numbers of mistakes in answering the multiple-choice questions after the completion of the donning or doffing steps were recorded by the computer simulation program. There were respectively 8 and 9 multiple-choice questions for the donning and doffing procedures. The statistics was shown in Table 5. A total of 43 mistakes were recorded for the 25 subjects, 10 made during the donning procedure and 33 at doffing. This means that on average the subjects scored 95% and 85% in the donning and doffing evaluation respectively. User Satisfaction Among the 19 items of the IMB CSUQ13, the score of each item as rated by the subjects ranged between 1 and 3 out of the 7-point Likert scale (lower score means better satisfaction). The lowest mean score was 1.4 (for four items) and the highest was 1.9 (for one item), while the standard deviations of the scores for the items were in the range of 0.49 to 0.78. The results showed that the subjects were satisfied with the computer simulation program and the rating was consistent among all the subjects in the experimental group. They agreed that the computer simulation program was easy to use.
Discussion In this study, it was hypothesized that computer-simulated training could improve the PPE donning and doffing skills of healthcare workers. Refer to the results in Table 2, by comparing the pre-test and post-test performance of the control and experimental groups respectively, it is clear that there was an improvement in donning and doffing skills within each group, suggesting that the conventional and computer-simulated training approaches were both effective. However, when the post-test donning and doffing performance between the two groups was compared, the experimental group indeed outperformed the control group which indicated that the use of the computer simulation program was able to further enhance the learning of proper PPE usage. On the other hand, after going through either training approach, all subjects were able to achieve the passing mark of 90% as required by the infection control department of the participating hospital. This demonstrates the importance of infection control training in raising healthcare workers’ competency in using PPE. While it is expected that healthcare workers of higher rank and with more experience would be able to achieve higher PPE donning and doffing score in the pre-test, the results from the correlation analysis (Table 3) showed that age, rank and working experience were all not significantly associated with the pretest score. That is, the competency of the healthcare workers in PPE donning and doffing was about the same regardless of their rank or nursing experience. Coupled with the fact that only a few of the subjects managed to get the passing mark before the training, the finding brings up the need for attention to raise the awareness of proper PPE usage. It is therefore important for healthcare organizations and nursing schools to provide appropriate PPE education, and the proposed computer-simulated training is a promising approach. On the other hand, the correlation analysis conducted with the post-test donning and doffing scores in
Table 4 reveals that the conventional training approach was better received by healthcare workers of higher rank. This may be attributed to the stronger work experience they have that enables them to better comprehend the skills conveyed in the conventional training approach than the lower-rank healthcare workers. This was not the case for the computer simulation program where the post-test score were not related with age, rank and working experience of the subjects, and thus a more suitable PPE training approach for healthcare workers in general while achieving a similar outcome. It appears that the subjects were less familiar with the doffing steps as evident from the fact that they made more errors in answering the multiple-choice questions presented by the computer simulation program on the doffing procedure when compared to that on the donning procedure. Moreover, one third of the mistakes were made in answering the questions concerning the removal of N95 respirator (Table 5). In the computer simulation program, the non-contact technique for removing N95 respirator was adopted. This is a new technique recently recommended by the local infection control authority aiming to minimize hand contamination due to the removal. The results showed that subjects were not accustomed to this technique. For example, the performance data logged in the web server showed that the subjects chose to grasp the bottom tie with one hand, instead of using both hands, as the first step of the removal of the N95 respirator (see Figure 3). Given the relatively weaker understanding of the doffing skills, more intensive training shall be provided accordingly to enhance the knowledge of proper PPE removal.
Limitations Despite a controlled trial and the favorable results, the sample size of the study was relatively small, involving only 50 subjects. If more subjects could be recruited from other hospitals, the reliability of the study would be enhanced. Stronger evidence could be made available to show that the computer simulation program was well suited for healthcare workers in general, independent of their rank or experience. Besides, the study lasted for 3 weeks for the experimental group and the subjects only received the computer-simulated training once. It would be useful to further investigate the virtual learning progress of the subject when they received the training multiple times, as well as the relationship between the intensity of the computerized training and the performance in actual PPE usage, i.e. the effectiveness of the transfer of knowledge gained from the computer-simulated training into real-world practice.
Conclusion The study has demonstrated the effectiveness of using the computer simulation program to facilitate the training of PPE donning and doffing skills. It is an effective way to complement and enhance the conventional PPE training for healthcare workers, and aid the strengthening of infection control and improving occupational health. This simulation program is a web-based application which is readily available and accessible online simply with a generic web browser. While the results of the study were promising, a large-scale study shall be conducted to further substantiate the training effectiveness, ensuring that the knowledge gained from the virtual training is well transferrable to proper PPE donning and doffing practice. In particular, subjects will be allowed to use the computer simulation program multiple times over an extended period so as to evaluate further their e-learning progress and to study the retention effect. The current
simulation program presented three-dimensional (3D) objects in two dimensions. To increase the virtual realism, a 3D version of the program will be developed to enable users to visualize the PPE and the simulated scenarios in a more intuitive way.
References 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13.
Conly JM. Personal protective equipment for preventing respiratory infections: What have we really learned? Canadian Medical Association Journal. 2006;175(3):263. Chan JTS, Lau, W. H. K., & Wu, Y. F. Confidence test for personal protective equipment. Hong Kong Journal of Emergency Medicine. 2002;9(4):195-200. Reid SM, Farion, K. J., Suh, K. N., Audcent, T., Barrowman, N. J., & Plint, A. C. Use of personal protective equipment in Canadian pediatric emergency departments. Canadian Journal of Emergency Medicine. 2011;13(2):71-78. Sax H, Perneger, T., Hugonnet, S., Herrault, P., Chraiti, M. N., & Pittet, D. Knowledge of standard and isolation precautions in a large teaching hospital. Infection Control and Hospital Epidemiology. 2005;26(3):298-304. Lau JTF, Fung KS, Wong TW, et al. SARS Transmission among Hospital Workers in Hong Kong Emerging Infectious Disease. 2004;10(2):280-286. Pang X, Zhu Z, Xu F, et al. Evaluation of control measures implemented in the severe acute respiratory syndrome outbreak in Beijing, 2003. Journal of the American Medical Association. 2003;290(24):3215. Strauss R, & Kinzie, M. B. Student achievement and attitudes in a pilot study comparing an interactive videodisc simulation to conventional dissection. American Biology Teacher. 1994;56:398-402. Weaver A. High fidelity patient simulation in nursing education: An integrative review. Nursing Education Perspectives. 2011;32(1):37-40. Cassidy CR, & Kreitner, R. Supervision: Setting people up for success. Mason, OH: Southwestern Cengage Learning; 2010. Infection prevention and control of epidemic- and pandemic-prone acute respiratory diseases in health care (WHO Interim Guidelines) 2007; http://www.who.int/csr/resources/publications/WHO_CDS_EPR_2007_6c.pdf. Guidelines on Infection Control Practice in the Clinic Setting. 2011; http://www.chp.gov.hk/files/pdf/guidelines_on_infection_control_practice_in_the_clinic_s etting_dec_2011.pdf. Polit DF, & Beck, C.T. Nursing Research: Principle and Methods. Philadelphia, PA: Lippincott; 2004. Lewis RJ. IBM Computer Usability Satisfaction Questionnaires: Psychometric Evaluation and Instruction for use. International Journal of Human Computer Interaction. 1995;7(1):57-78.
List of Figures Figure 1. Snapshots of the computer simulation program: (a) user is dragging the N95 respirator toward the virtual healthcare worker, (b) a multiple choice question about the usage of N95 respirator is shown, (c) the system prompts the user for having mistakenly put a cap on the worker right after wearing the N95 respirator (should first put on the gown instead), (d) user clicks on the glove to remove it, (e) a multiple choice question about the removal of the glove is shown, (f) user is dragging the glove to the trash bin with a lid. Figure 2. Research design. Figure 3. Subjects picking ‘C. Grasp the bottom tie with one hand’ as the first step to be performed for remove the N95 respirator while the correct answer is ‘D. Grasp the bottom tie with both hands’.
List of Table Table 1 Demographic data (percentage in parentheses) Table 2 PPE donning and doffing evaluation score Table 3 Correlation analysis (spearman’s rho) of pretest score and demographic variables Table 4 Correlation analysis (spearman’s rho) of posttest score and demographic variables Table 5 Mistakes in answering multiple choice questions
Figure
Figure 1. Snapshots of the computer simulation program: (a) user is dragging the N95 respirator toward the virtual healthcare worker, (b) a multiple choice question about the usage of N95 respirator is shown, (c) the system prompts the user for having mistakenly put a cap on the worker right after wearing the N95 respirator (should first put on the gown instead), (d) user clicks on the glove to remove it, (e) a multiple choice question about the removal of the glove is shown, (f) user is dragging the glove to the trash bin with a lid.
Figure 2. Research design.
Figure 3. Subjects picking ‘C. Grasp the bottom tie with one hand’ as the first step to be performed for remove the N95 respirator while the correct answer is ‘D. Grasp the bottom tie with both hands’.
Table
Table 1 Demographic Data (Percentage in Parentheses)
Characteristic Age
Rank
Nursing working experience
Experimental group (n = 25) 11 (44%) 9 (36%) 5 (20%) 6 (24%) 5 (20%) 14 (56%) 5 (20%) 6 (24%) 1 (4%) 13 (52%)
Range 20-30 31-40 41-50 Registered nurse Enrolled nurse Healthcare assistant 0-3 years 4-6 years 7-9 years Above 9 years
Control group (n = 25) 7 (28%) 9 (36%) 9 (36%) 6 (24%) 5 (20%) 14 (56%) 10 (40%) 2 (8%) 0 (0%) 13 (52%)
Table 2 PPE Donning and Doffing Evaluation Score Procedure
Donning Doffing
Experimental group Time Pre Post Pre Post
Mean 13.52 15.08 17.76 19.48
SD p 0.653 0.000 0.493 0.663 0.000 0.653
Control group Mean 13.60 14.56 17.28 18.32
SD p 0.913 0.000 0.821 0.980 0.003 0.988
Between groups p 0.859 0.013 0.055 0.000
Table 3 Correlation Analysis (Spearman’s rho) of Pretest Score and Demographic Variables Variable Pretest score
Pretest score --
Age
Rank
Experience
Age
-0.117
--
Rank
-0.069
-0.506**
--
Experience
-0.180
0.706**
-0.443*
--
Note. Pretest score = pretest score of donning and doffing evaluation *p < .05. **p < .01
Table 4 Correlation Analysis (Spearman’s rho) of Posttest Score and Demographic Variables
Experimental group
Control group
Variable Posttest score
Posttest score ---
Age
Age
0.30
--
Rank
0.203
-0.375
--
Experience
-0.184
0.789**
-0.397*
Posttest score
Rank
--
--
Age
0.462*
--
Rank
-0.563**
-0.679**
--
0.133
0.731**
-0.475*
Experience
Experience
Note. Posttest score = posttest score of donning and doffing evaluation *p < .05. **p< .01
--
Table 5 Mistakes in Answering Multiple Choice Questions Procedure Donning
Doffing
Step Wear N95 respirator Wear face shield Wear cap Wear gown Wear gloves Remove gloves Remove gown Remove cap Remove face shield Remove N95 respirator
No. of times 3 1 4 2 0 4 5 8 5 11