Measures of Student Competence Following a Patient-Centered Project
3
ARTICLES Measures of Student Competence Following Participation in a PatientCentered Medical Home Demonstration Project-Practicum in Primary Care Sandi J. Lane, PhD, FACHE, LNHA Abstract
The Health Care Management Program at a regional university located in the Southeast, in collaboration with the lead agency for a federally sponsored Multipayer Advanced Primary Care Demonstration Project (MAPCP), developed a practicum in primary care. The practicum allowed undergraduate students to gain experience while assisting clinics in reframing their processes to meet National Committee on Quality Assurance (NCQA)-Patient-Centered Medical Home (PCMH) recognition standards. We analyzed student and clinic staff member’s perceptions of student competence following the practicum experience using 12 of the 26 competencies from the National Center for Healthcare Leadership (NCHL) competency model v2.1. Following their practicum experience, students rated all but communication skills, interpersonal understanding, and organizational awareness competencies as important (4) or very important (5) to their career. Students’ perceived the greatest gain in the competencies of collaboration and professionalism (mean=4.4) and the lowest gain in change leadership and interpersonal understanding (mean=3.8). Clinic staff rated students highest on collaboration (mean=4.8), followed by relationship building and information technology (mean=4.6), and lowest on change leadership skills (mean=3.9). In most of the competencies evaluated, similarities were observed between the students’ perceived gain in competence and clinic staff’s rating of students’ competence. Collaboration between universities and health
Please address correspondence to: Sandi J. Lane, PhD, FACHE, LNHA, Department of Nutrition and Health Care Management, Appalachian State University Box 32168, Boone, NC 286082168, Email:
[email protected], Phone: (828) 262-7482.
4
The Journal of Health Administration Education
Winter 2014
services organizations/agencies enhance experiential learning opportunities for undergraduate students and should be further explored.
Introduction
Active learning strategies are often used to promote student learning and increase retention of theories and concepts (Fink, 2003). Faculty from many disciplines frequently use case studies, exercises, and simulations in their classroom teachings to engage students and provide opportunities to apply concepts and theories. However, these in-class activities cannot provide the real experiences students need to prepare them for the turbulent healthcare environment (Hartman & Crow, 2002). Immersion in experiential learning situations allows undergraduate students to apply the concepts learned in the classroom to real situations (Goodman, 2003). Undergraduate healthcare management students are often introduced to the realities of the complex healthcare environment through the experiential learning of their internship and/or practicum. Experiential learning experiences are believed to be so important to building an undergraduate healthcare management student’s competence that many programs require students to complete an internship. In fact, the Association of University Programs in Health Administration (AUPHA) requires student internships for programs choosing certification (AUPHA, 2012). This article describes the processes used to implement an undergraduate healthcare management practicum in primary care (practicum), then explores and examines each party’s perception of student competency using 12 of the 26 competencies from the National Center for Healthcare Leadership (NCHL) Competency Model. One unique aspect of our study was the facilitation model employed to implement the practicum experience. Community Care of North Carolina (CCNC), the lead organization of a three-year Multi-payer Advanced Primary Care Demonstration Project (MAPCP) sponsored by U.S. Department of Health and Human Services and the Centers for Medicare and Medicaid Services in collaboration with an undergraduate healthcare management program, designed the facilitation model and created the practicum. The conceptual model is guided by the work of Goodman (2003) and Dalston (2004), who posit that experiential experience is critical to academic learning and healthcare management competency development. Our specific aims were to determine the healthcare management competencies the students perceived they gained from participating in the practicum, as well as the healthcare management competencies the clinic staff believed the students brought to their clinic.
Measures of Student Competence Following a Patient-Centered Project
Background
5
The value and necessity of experiential learning to competency development in graduate health administration programs is well documented (Fine, 2001; White, 2002). As a result, experiential learning is universally endorsed as an important curricula component of Commission on Accreditation of Healthcare Management Education accredited programs (www.cahmeweb.org). However, the literature is sparse in the study of experiential learning in undergraduate programs preparing entry-level healthcare managers. One recent study assessed the role of an internship in undergraduate student competency development and found internships were critical for competency development in the domains of interpersonal/human relations, conceptual/critical thinking, technical, and personal growth and development (Thompson, 2005). However, a review of the literature revealed a gap in the area of undergraduate student competency development during a practicum. During an internship, healthcare management students participate in various activities such as attending meetings, shadowing providers and managers, observing work flow, participating as team members, and oftentimes completing projects. The specific activities and experiential learning of an internship are determined by students’ career interests, the type of host healthcare organization, the preceptor’s role within the organization, and organizational needs at the time of the internship. Therefore, student experiential learning during internships is diverse and competency development varies depending upon the individual student experience. The benefits of internships as action-learning are well documented in the literature (Cook, Parker, & Pettijohn, 2004; Gault, Redington, & Schlager, 2000; Knouse, Tanner, & Harris, 1999; Thompson, 2005). Other forms of experiential learning, such as residencies, fellowships and practicums, are infrequently found in undergraduate healthcare management programs. Residencies and fellowships, typically found in graduate healthcare management programs, are multisemester experiential learning opportunities offered after the successful completion of required coursework. Although practicum experiences are often used in health sciences, teaching, and foreign language curricula, they are not typical in business or management baccalaureate programs. During a practicum, students work in a specified area of study to practice classroom concepts in the real-world environment. Merriam-Webster defines “practicum” as the “supervised practical application of previously studied theory.” The practicum in primary care designed for this study offered structured opportunities for students to apply the theories and concepts learned in the classroom under the supervision of a team of preceptors. The predefined tasks and activities of the practicum were determined by the focused outcome of NCQA-PCMH recognition of the participating clinics. The
6
The Journal of Health Administration Education
Winter 2014
tasks included developing organizational policies and procedures, assessing and tracking workflows, implementing new technology, and monitoring the effectiveness of an organization’s processes. During the practicum, students worked as members of their clinic, taking ownership of and completing specific tasks – a more participatory experience than the observing and shadowing experience of a traditional internship. Through experiential learning experiences, students gain the knowledge, skills, and abilities (often called competencies), necessary for successful careers in healthcare management. During the past two decades, healthcare administration faculty, industry practitioners, and professional associations have each developed competencies and/or competency models by which student learning and healthcare management practice are measured (Bradley et al., 2008; Calhoun, Davidson, Sinioris, Vincent, & Griffith, 2002; Campbell, Lomperis, & Arrington, 2006; Dye & Garman, 2006; Finstuen & Mangelsdorff, 2006; Robbins, Bradley, & Spicer, 2001; Shewchuk, O’Connor, & Fine, 2006; Stefl, 2008; White & Begun, 2006). Some models and assessment tools were developed for a specific population or focus (e.g., graduate students, seniorlevel executives, or medical-group management professionals), while others were developed for general healthcare administration fields and various stages of career growth. Of the many models and assessment tools developed, two examples were developed through collaborations/consortiums with diverse stakeholder involvement, and therefore, deserve mention. The first model developed through a consortium is the National Center for Healthcare Leadership (NCHL) Competency Model. The NCHL Competency Model places 26 identified competencies into three domains: Transformation, Execution, and People. Each competency is scaled across career stages identified as levels (1 = entry-level to 5 = advanced careers). The NCHL model was developed using knowledge gained from extensive academic research, interviews with experts in the field, behavioral interviewing, psychometric analysis, and pilot-testing surveys (Calhoun et al., 2008). The second model is the Healthcare Leadership Alliance (HLA) Competency Model. The HLA Competency Model utilizes the five domains of Communication and Relationship Management, Leadership, Professionalism, Knowledge of the Healthcare Environment, and Business Skills and Knowledge. It was developed from the HLA consortium member organizations’ credentialing processes and delineates the competencies that were common among the consortium members (Stefl, 2008). Both models place leadership at the core with the competency domains surrounding and contributing to successful leadership, similar to how the spokes of a wheel support the hub enabling a wheel to turn. The NCHL Competency Model allows for the scaling of competency assessment according to
Measures of Student Competence Following a Patient-Centered Project
7
career stages, including entry level, whereas the HLA uses credentialing-level criteria, which often requires experience in the discipline. Since participants in the present study were undergraduate students, the NCHL Competency Model was used to assess competency following the practicum experience.
Methods
Student Experiential Learning – The Practicum in Primary Care The Health Care Management (HCM) Program at a regional university in the Southeast developed the practicum in collaboration with CCNC’s AccessCare of the Blue Ridge (AccessCare). The practicum was an academic credit-bearing course that provided real-life healthcare management experience in primary care clinics beginning fall 2011. The practicum course was led by a HCM faculty and AccessCare’s Patient-Centered Medical Home leadership team (AccessCare’s leadership team). Both groups acted as facilitators between the students and clinic staff. AccessCare’s leadership team included a CCNC physician consultant with over 20 years of primary care experience, a nurse case manager who had worked closely with most of the practices in the region, an administrative coordinator familiar with AccessCare projects, and an information system technologist who has lived most of his life in this region. Student experiences included modifying and writing policies and procedures, using medical office technology, building relationships with clinic staff, leading change initiatives, and assessing operational performance. The focus of the practicum was to assist the primary care clinics in achieving National Committee on Quality Assurance-Patient-Centered Medical Home (NCQA-PCMH) recognition using the 2011 standards. Encouragement for clinics to meet 2011 NCQA-PCMH standards came from the three-year MAPCP project sponsored by the U.S. Department of Health and Human Services and the Centers for Medicare and Medicaid Services. CCNC led the implementation of MAPCP in three rural counties. Implementation of MAPCP required the primary care clinics to reframe their operations to meet 2011 NCQA-PCMH recognition standards, an arduous and daunting task for rural clinics with a skeleton staff. The NCQA-PCMH model requires clinicians to build partnerships with their patients and families to insure they receive the care when and where they need it through the use of information technology, health registries, and culturally and linguistically appropriate communication (NCQA, 2011). Students in the HCM program and the pre-professional sciences interested in helping the clinics obtain NCQA-PCMH recognition could enroll in the practicum. A total of five students were enrolled during the fall of 2011; ten in the spring of 2012 (seven new, three returning); six in the summer of 2012
8
The Journal of Health Administration Education
Winter 2014
(four new, two returning); and six in the fall of 2012 (five new, one returning). Students were enrolled for one semester at a time and could enroll for up to two semesters for a total of six credits. Students were expected to attend weekly class meetings and establish a mutually agreeable work schedule with the manager of their clinic. One of the first assignments was for each student to prepare a PowerPoint presentation introducing themselves and the MAPCP to the clinic staff. Preparing a PowerPoint presentation required the student to become familiar with the NCQA-PCMH standards and their role in the clinic’s process of achieving NCQHA-PCMH recognition. Students were encouraged to identify “PCMH Champions” within the practice and meet with them regularly to discuss progress, problems, and concerns. Each semester began with a meeting to introduce the students to AccessCare leadership team members and HCM faculty, and to review the student’s roles and responsibilities during the practicum. During this meeting, a member of the AccessCare leadership team led a discussion on Health Insurance Portability and Accountability Act (HIPAA) compliance and the expectation that students would adhere to patient confidentiality guidelines. Students signed HIPAA compliance and Business Associate Agreements. The students were then assigned to a practice, provided with NCQA-PCMH resources, and asked to review the 2011 PCMH Workbook and training webinars produced by CCNC. In addition, a website was built for the practicum students hosting their syllabus, core documents, key contact information, helpful web links, a shared calendar, and a place to post and share their work. The practicum schedule required the students to attend class meetings and work in their clinic each week. During the class meetings, the students learned about the Standards, Elements, and Factors of the 2011 NCQA-PCMH Recognition Process, including best practices and overcoming implementation challenges, HIPAA compliance, and relationship-building techniques. The class meeting time provided an opportunity for students to share experiences and learn from each other. Students were expected to work 8-10 hours each week on the practicum during the academic school year and 40 hours each week during the summer semester. This time was divided between in-practice activities (e.g., communicating with the practice staff on task assignments, and observation of practice processes and activities), and time outside of the practice writing policies, flowcharting work processes, and developing spreadsheets. In addition to the weekly class meetings, facilitators met with students individually, when requested, to discuss various implementation challenges, including concerns that the students could not or did not feel comfortable resolving on their own. For example, facilitators provided clarification on program requirements and specific detail on how to upload documents and/
Measures of Student Competence Following a Patient-Centered Project
9
or pay for an application. Students had the independence and autonomy to implement processes in collaboration with their clinic managers, while AccessCare facilitators were available to provide leadership and direction. Assessment of Student Learning Using the NCQA-PCMH standards as a guide, 12 competencies relevant to the student task performance were selected from the NCHL Competency Model (Table 1). Although the NCHL Competency Model was designed to identify and measure mastery of healthcare leadership competencies for participants in graduate education programs and professional development programs, many of the core competencies are applicable for measuring undergraduate student learning following an experiential learning experience. The NCHL Competency Model defines competency as behavioral and technical characteristics that differentiate levels of leadership performance across career stages. Within each competency, only the entry level (level 1) was utilized because undergraduate students are pre-entry into the workforce. Students were expected to use skills from multiple competencies found in each of the domains while participating in the practicum. Competence was measured in three ways: from the clinic staff perspective; from student perspective of the importance of the competency to their career; and student perceived gain in competency from the practicum experience. We used questions on student achievement of the 12 competencies to both interview clinic staff and also survey the students. Institutional Review Board approval was obtained to conduct this study from the sponsoring university’s Office of Research Programs. Data Collection and Sample Fourteen clinics in three counties participated in the MAPCP project and used HCM students to assist them in achieving NCQA-PCMH recognition status. Participating clinics received a letter of agreement requesting participation in the study and 12 agreed to participate. Interviews were scheduled with one staff member from each clinic who worked closely with the HCM student(s). The semi-structured interviews were conducted at a mutually agreeable time and held in a private office at the clinic. Clinic respondents were asked about their involvement with – and their initial perception of – the MAPCP project, information on clinic operations (e.g., the number of providers and support staff), use of electronic or paper health records, type of patient scheduling (e.g., electronic or paper-based), availability of same-day appointments, and current level of PCMH recognition (if submission complete). Respondents were also asked to assess student achievement of the 12 competencies on a five-point Likert scale (5 = very competent and 1 = limited or no competency). During the
10
The Journal of Health Administration Education
Winter 2014
interview, the principle investigator recorded the rating score for each of the students as determined by the respondent. In addition, interviewees were also asked to discuss their opinions about the student’s contribution to their clinic achieving NCQA-PCMH recognition. Table 1 Domains and 12 Competencies used to Assess Student Competency
Domain
Competency
Level 1 Competency Tasks
Transformation
Accountability
Communicates requirements and expectations through directions and the understanding of task requirements
Achievement orientation
Tries to do the job well, expresses a desire to do better
Analytical thinking
Understands a situation, issue, or problem by breaking it into smaller pieces
Community orientation
Keeps stakeholders informed of project progress, follows through when asked
Change leadership
Identifies areas where change is needed or what needs to be changed
Collaboration
Conducts work in a cooperative manner, supportive of team decisions
Communication skills
Speaks and writes in a clear and logical manner, (i.e., prepare written policies)
Execution
Information techRecognizes the potential of information sysnology management tems in process and patient service improvement, actively promotes information system implementation
People
Organizational awareness
Understands and uses the formal structure to get things done, (i.e., chain of command)
Interpersonal understanding
Recognizes emotions and concerns of others, and understands unspoken thoughts or feelings.
Professionalism
Demonstrates ethics, social accountability, and acts openly and honestly
Relationship building
Establishes, builds, and sustains professional contacts in order to build a professional network of peers with similar interests
Students were surveyed between September 2012 and December 2012 using the electronic survey tool SurveySelect. Students enrolled December 2011 through August 2012 were surveyed between October 2012 and Decem-
Measures of Student Competence Following a Patient-Centered Project
11
ber 2012. Students enrolled in the practicum for the first time in the fall of 2012 were surveyed in December 2012. In all, 11 of the 22 students took the survey, with 10 completing all of the questions. Emails with a hyperlink to SurveySelect inviting students to participate in the study were sent twice. Student survey questions included: demographic information (e.g., age, gender, race/ethnicity), number of semesters enrolled in the practicum, the reason for enrollment, and the type of activities participated in. Survey questions asked students to rate the importance of the 12 selected competencies for their careers in healthcare management, as well as the degree to which the practicum contributed to their competency in each of the areas. The survey utilized the same five-point Likert scale used in the preceptor interviews. In addition, students who had completed both an internship and the practicum were asked to rate the differences between the two in areas such as level of ease, amount of work expected of them, level of responsibility, interaction with staff, leadership of a team, and responsibilities as a coworker. Table 2 Student Demographics Age (mean)
23.2
Gender Male 4 Female 6 Race/Ethnicity Caucasian 8 Hispanic/Latino 2 Completed an internship prior to enrolling in the Practicum (n)
3
Practicum was student’s internship (n)
4
Hours worked in clinic (mean)
10.5
Hours worked on Practicum outside of clinic (mean)
11.1
Note: n=10 students
12
The Journal of Health Administration Education
Results
Winter 2014
The ten students who completed the survey were, on average, 23 years old: six were females, eight were Caucasian, and two were Hispanic/Latino. Three students reported completion of the program’s required internship prior to participating in the practicum, and four reported that they were participating in the practicum in lieu of the internship. On average, the students worked 10 hours each week in their clinic and 11 hours outside of the clinic on projects assigned by their clinic manager (Table 2). Students reported participating in similar activities during the practicum. For example, all ten students reported that they wrote policies, nine of the students educated staff on NCQA-PCMH guidelines and assessed clinic work flow, and eight students developed processes and forms. In contrast, only two students reported working as a staff member (e.g., answering phones, data entry, etc.) and only one attended staff training. Students believed that 9 of the 12 competencies were either important or very important to their careers as healthcare mangers (range = 4.0-5.0), with accountability and collaboration having the highest mean (4.8). Interpersonal understanding had the lowest mean (4.3) and the widest range (2.0-5.0). The importance of communication (mean=4.6) and organizational awareness (mean=4.4) competencies were rated as neutral to very important (3.0-5.0) (Table 3). The perceived gain in competencies following participating in the practicum demonstrated greater variation than importance of the competencies to their career. Relationship building was the only competency where students felt the practicum either prepared (4.0) or highly prepared (5.0) them for their careers. Whereas, on average, students reported the highest gain in the competencies of collaboration (mean = 4.4), professionalism (mean = 4.4), and relationship building (mean = 4.3). Students reported the lowest average competency growth in change leadership and interpersonal understanding, both yielding a mean of 3.8. Turning to clinic staff’s rating of student competency, clinic staff scored the students highest on collaboration (mean = 4.8), information technology management (mean = 4.6), and relationship building (mean = 4.6). Student competencies rated the lowest by clinic staff included change leadership (mean = 3.8), accountability (4.1), and organizational awareness (4.1). One manager commented that she would not expect students at this level of their career to be competent in change management. Six students responded to an open-ended question asking them to describe the most important knowledge and skills gained from participating in the practicum. The responses were notably similar and focused on applica-
Measures of Student Competence Following a Patient-Centered Project
13
tion of knowledge and skills in real situations and implementation of national guidelines such as NCQA-PCMH. Table 3 Assessment of Competency: Student’s Perceived Importance, Student’s Perceived Gain, and as Rated by Clinic Staff
NCHL Competency
Student perceived importance of competency
Student perceived gain in competency
n=10
Average student competency rated by clinic staff
n=10
n=12
mean
range
mean
range
mean
range
4.8
4.0-5.0
4.1
2.0-5.0
4.1
1.0-5.0
Achievement Oriented
4.5
4.0-5.0
4.2
2.0-5.0
4.2
1.0-5.0
Analytical Thinking
4.6
4.0-5.0
4.0
2.0-5.0
4.3
1.0-5.0
Accountability
Change Leadership
4.6
4.0-5.0
3.8
2.0-5.0
3.9
1.0-5.0
Collaboration
4.8
4.0-5.0
4.4
2.0-5.0
4.8
3.0-5.0
Communication
4.6
3.0-5.0
4.2
3.0-5.0
4.1
1.0-5.0
Community Orientation
4.6
4.0-5.0
4.0
2.0-5.0
4.3
2.0-5.0
Information Technology Management
4.6
4.0-5.0
4.1
2.0-5.0
4.6
2.0-5.0
Interpersonal Understanding
4.3
2.0-5.0
3.8
2.0-5.0
4.3
1.0-5.0
Organizational Awareness
4.4
3.0-5.0
4.1
3.0-5.0
4.1
1.0-5.0
Professionalism
4.7
4.0-5.0
4.4
3.0-5.0
4.6
2.0-5.0
Relationship Building
4.7
4.0-5.0
4.3
4.0-5.0
4.6
2.0-5.0
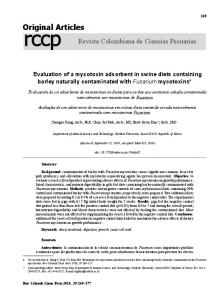
Perception of the differences between an internship and the practicum were rated by six of the ten students, who reported that during the practicum a greater volume of work and a higher level of responsibility were expected as compared to an internship. The practicum experience also provided more opportunities to lead teams and workgroups. In contrast, they indicated the internship was easier. In the practicum, they interacted with clinic staff more and had greater responsibilities as a coworker (Figure 1).
14
The Journal of Health Administration Education
Winter 2014
Figure 1 Student Perception of Differences Betweeen Practicum and Internship
Note: n=6 students
Discussion
Using 12 competencies from the NCHL Competency Model, this study assessed student perception of the importance of competencies; students’ self-assessment of growth; and clinic staff’s rating of student competence following a practicum in primary care. Students perceived they had the greatest growth in the competencies of collaboration, professionalism, and relationship building from their practicum experiences. Clinic managers rated the students similarly, with collaboration, information technology management, and relationship building having the highest average. Change leadership was the lowest-rated competency, both in terms of students’ perceived growth and clinician evaluation, findings one might expect as there is little opportunity for students to lead change at this point in their career. Writing policies for new processes or designing work flows to meet 2011 NCQA-PCMH guidelines required students to become familiar with clinic operations. Successful integration of students in clinic operations required them to collaborate and build relationships with clinic staff to understand clinic processes and establish ways to implement the 2011
Measures of Student Competence Following a Patient-Centered Project
15
NCQA-PCMH standards. Development of students’ collaboration skills may have resulted from them functioning as part of the team and working alongside the clinic staff to achieve the goal of NCQA-PCMH recognition. Collaboration is critical when implementing systematic changes to clinic operations. Cooperating with team members, keeping others informed and advised on project status, and maintaining a positive attitude are critical dispositions for successful collaboration. Student perceived growth in professionalism could stem from this being their first experience as an accountable member of a healthcare team. In addition, perceived growth in professionalism could be attributable to the students’ desire to act consistently and in accordance with the organization’s core values. These findings are consistent with what students reported during informal discussions. Students reported no gain in information technology skills from the practicum experience, yet clinic managers rated students competent on this measure. This may not be surprising as the students were younger (23.2 years old, on average) than most of the clinic staff members and could offer the technology skills they used every day while in school or at home. Clinic staff reported student skills in developing spreadsheets and using the electronic health record system were integral to clinic achievement of NCQA-PCMH recognition. Using a triangulation approach to assess competencies provided an opportunity to examine student competency from three perspectives: the student’s perceived importance of the competency to their career; the student’s perceived growth in competency from participating in the practicum; and the clinic manager’s rating of student’s competence. Correlations between students’ perceptions and clinic manager ratings of competence were observed for collaboration and relationship building. Assessing competency from multiple perspectives provides additional insight into the evaluation of student outcomes following experiential learning and deserves further study. Landry and colleagues studied competency training of healthcare leaders, asking: 1) whether competency training matters; and 2) whether advancement/ career success impacts their self-perceived competence. They reported that healthcare executives who received training perceived themselves as more competent compared to their peers without training opportunities (Landry, Stowe, & Haefner, 2012). The students may perceive the practicum as a form of training and therefore rate a gain in competence following the practicum experience. The 2011 NCQA-PCMH standards are complex and often burdensome for clinics to implement. The students’ dedication to learning the standards and best practices in enough depth to apply them may be due to the perceived value of the experience to their career. Research indicates that the more important an individual believes the competency is to their success, the more willing they are
16
The Journal of Health Administration Education
Winter 2014
to learn it and dedicate time to improving it (Maurer, Kimberly, Heather, Stuart, & William, 2003). Although the students believed all the competencies were important or very important to their careers, perceived gain in competency was rated highest for collaboration and professionalism. It is unknown whether this is due to the students’ goal orientation, their desire to improve these competencies, or their perceived ability to learn and improve them. Further research to parse out factors contributing to individual perceptions of competency development to career success will contribute to competency training opportunities. This study’s limitations include its small sample size both in the number of students (10) and clinics (12) including three of the practices under a central coordinator for the NCQA-PCMH submission. The small sample of students and the wide range of values for each of the competencies limit the use of the means. The collaboration between the AccessCare’s leadership team and HCM faculty was critical to the success of this practicum, limiting the ability to generalize and apply the findings to experiential learning experiences with similar leadership resources. Unlike an internship, a requirement for all HCM students, students applied and were selected to participate in the practicum – a requirement for all HCM students; unobserved differences between these students and other students are unknown. Practices were invited to participate in the collaborative and subsequently this study; unobserved differences between these practices and others are unknown.
Conclusion and Implications
The practicum guided by a collaborative between AccessCare’s leadership team and HCM faculty provided a valuable experiential learning experience for undergraduate students. Student involvement in a practice’s transformation of operations and subsequent achievement of NCQA-PCMH recognition provided opportunities to gain competence and practice concepts and theories learned in the classroom. Overall, students believed these competencies were important for their career success and the practicum provided an opportunity to improve many of them. Collaboration between universities and health services organizations/agencies enhances experiential learning opportunities for undergraduate students and should be explored further.
References
Association of University Programs in Health Administration (AUPHA) (2012). Guidelines for Undergraduate Certification Criteria. Retrieved May 15, 2013,from http://www.aupha.org/files/public/Guidelines%20for%20Under graduate%20Certification%20Criteria%202012%2B%2B.pdf
Measures of Student Competence Following a Patient-Centered Project
17
Bradley, E. H., Cherlin, E., Busch, E., Epstein, A., Helfand, B., & White, W. D. (2008). Adopting a competency-based model: Mapping curricula and assessing student progress. Journal of Health Administration Education, 25(4), 37-50. Calhoun, J. G., Dollett, L., Sinioris, M. E., Wainio, J. A., Butler, P. W., Griffith, J. R., & Warden, G. L. (2008). Development of an interprofessional competency model for healthcare leadership. [Research Support, Non-U.S. Gov’t]. Journal of Healthcare Management, 53(6), 375-389; discussion 390-371. Calhoun, J. G., Davidson, P. L., Sinioris, M. E., Vincent, E. T., & Griffith, J. R. (2002). Toward an understanding of competency identification and assessment in health care management. Quality Management in Health Care, 11(1), 14-38. Campbell, C. E., Lomperis, A. M., & Arrington, B. (2006). Competency-based healthcare management education: The Saint Louis University experience. Journal of Health Administration Education, 23(2), 135-168. Cook, S. J., Parker, R. S., & Pettijohn, C. E. (2004). The perceptions of interns: A longitudinal case study. Journal of Education for Business, 79(3), 179-185. Dalston, J. (2004). Core Leadership Concerns. Modern Healthcare, 34(22), 22. Dye, C. F., & Garman, A. N. (2006). Exceptional leadership: 16 critical competencies for healthcare executives. Chicago, IL: Health Administration Press. Fine, D. J. (2001). Experiential learning in health care administration. Journal of Health Administration Education (Special Issue), 107-116. Fink, I. D. (2003). Creating significant learning: Designing the learning we want into the student experience. NEA Higher Education Advocate, 20, 5-7. Finstuen, K., & Mangelsdorff, A. D. (2006). Executive competencies in health care administration: Preceptors of the Army Baylor University graduate program. Journal of Health Administration Education, 23(2), 199-215. Gault, J., Redington, J., & Schlager, T. (2000). Undergraduate business internships and career success: Are they related? Journal of Marketing Education, 22(1), 45-53.
18
The Journal of Health Administration Education
Winter 2014
Goodman, G. R. (2003). The occupation of health care management: Relating core competencies to growth as a distinct profession. Journal of Health Administration Education, 20, 147-165. Hartman, S. J., & Crow, S. M. (2002). Executive development in health care during times of turbulence. Journal of Management in Medicine, 16(5), 359-370. Knouse, S. B., Tanner, J. T., & Harris, E. W. (1999). The relation of college internships, college performance, and subsequent job opportunity. Journal of Employment Counseling, 36(1), 35. Landry, A. Y., Stowe, M., & Haefner, J. (2012). Competency assessment and development among health care leaders: Results of a cross-sectional survey. Health Services Management Research, 25(2), 78-86. doi:10.1258/hsmr.2012.01.2012 Maurer, J. T., Kimberly, A. W., Heather, R. P., Stuart, A. T., & William, C. C. (2003). Beliefs about ‘improvability’ of career-relevant skills: Relevance to job/rank analysis, competency modeling, and learning orientation. Journal of Organizational Behavior, 24, 107. Merriam-Webster (n.d.). Practicum - Definition and More from the Free Merriam-Webster Dictionary. Retrieved from http://www.merriam-webster.com/dictionary/practicum National Center for Healthcare Leadership (n.d.). National Center for Healthcare Leadership Competency Model version 2.1. Retrieved June 22, 2013, from http://www.nchl.org National Center for Quality Assurance (NCQA) (n.d.). 2011 Patient-Centered Medical Home (PCMH) Standards and Guidelines. Retrieved June 5, 2012, from http://www.ncqa.org/Programs/Recognition/PatientCenteredMedic alHomePCMH.aspx Robbins, C. J., Bradley, E. H., & Spicer, M. (2001). Developing leadership in health care administration: A competency assessment tool. Journal of Healthcare Management,46(3), 188-199.
Measures of Student Competence Following a Patient-Centered Project
19
Shewchuk, R. M., O’connor, S. J., & Fine, D. J. (2006). Bridging the gap: Academic and practitioner perspectives to identify early career competencies needed in health care management. Journal of Health Administration Education, 23(4), 367-392. Stefl, M. E. (2008). Common competencies for all health care managers: The health care leadership alliance model. Journal of Healthcare Management, 53(6), 360-374. Thompson, J. M. (2005). Competency development and assessment in undergraduate health care management programs: The role of internships. Journal of Health Administration Education (Fall 2005), 417-433. White, K. R., & Begun, J. W. (2006). Preceptor and employer evaluation of health administration student competencies. Journal of Health Administration Education,23(1), 53-68. White, K. R. (2002). Experiential learning in health administration: A new approach for new times. Journal of Health Administration Education, 20(2), 101-111.