Successfully Transitioning a Ventilator Dependent Spinal Cord Injured Patient to Eating 14 Months Post Injury – A Case Presentation Sarah Morgan & Jackie McRae Adult Speech and Language Therapy Service, London Spinal Cord Injury Centre Contact: Sarah Morgan,
[email protected]
Background – A hidden complication
Outcomes:
• Cervical spinal cord injury (CSCI) is a complex condition affecting multiple body systems. • Paralysis of some or all respiratory muscles will necessitate mechanical ventilation via tracheostomy.1 • Respiratory complications are the leading cause of morbidity & mortality in SCI • Ineffective cough, pulmonary infections, prolonged weaning and hypersecretions are common. • Incidence of dysphagia following CSCI is estimated to be around 40%2 • Dysphagia exacerbates complications and increases hospital length of stay by up to 50%.3 • With high rates of silent aspiration, clinical presentation is subtle, difficult to diagnose & poses a challenge to rehabilitation. • Eating, drinking and speaking are important patient goals and paramount to rehabilitation and reintegration. Clinical evidence suggests diverse decision making with regards to commencing oral intake.
Secre3on Ra3ng (Murray)
PAS Score
Swallow outcome Ven3la3on/ Tracheostomy status
On admission FEES Level 3
Thin fluids-‐8 SoO solids -‐8
Nil by mouth, daily swallow rehab, respiratory wean, cuff defla5on trials
Videofluoroscopy (at 2 Months)
Thin fluids-‐ 8 Yoghurt-‐ 3 SoO solids-‐3
Daily swallow trials with soO solids. Prompted second swallow
Route of nutri3on Method of communica3on
Vent dependent, Enteral feeding via cuff inflated 24/7. PEG tube. Nil by Size 8 Portex mouth suc5onaid. Forced vital capacity: 650mls
Non-‐verbal, exploring alterna5ve communica5on aids
Introduction: • We report a case of a 43 year old patient who sustained a CSCI and brain injury following resection of a subependymoma C3-T3 spinal tumor. He required a tracheostomy with ventilation and spent 14 months in a number of acute and rehabilitation settings with a diagnosis of intractable oropharyngeal dysphagia. He was admitted to the London Spinal Cord Injury Centre (LSCIC), for a specialist rehabilitation admission 4.
Enjoying cake with the tracheostomy team (with permission)
Approaches:
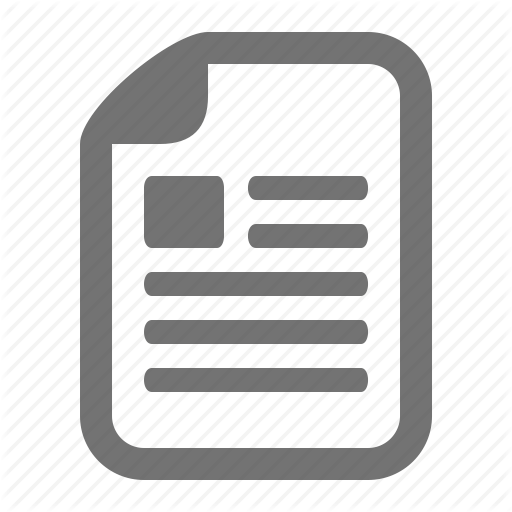
• Laryngeal weaning process (see figure 1) combines early cuff deflation alongside respiratory weaning to facilitate laryngeal sensation, speech and cough function, even in permanently ventilated patients. • Fibre-optic endoscopic evaluation of swallowing (FEES) allows direct visualisation of the pharynx and larynx to test sensation and motor functions. This allows assessment of responses to secretion clearance, cuff deflation, speaking valve and oral trials. • Baseline measures: Secretion rating scale (Murray 1999); PAS (Rosenbek, 1996). Forced vital capacity (FVC’s) • Daily swallow rehabilitation for 1 hour. To include principals of facial oral tract therapy (F.O.T.T); saliva swallows, chewing practice, modified shaker. Patient education, biofeedback and rigorous oral hygiene regimes.
Laryngeal Wean - change vent to allow cuff leak
Pressure support ≤ 20cmH2O (pressure controlled ventilation)
Tracheostomy with partial cuff deflation, whilst ON vent + swallow therapy programme.
Reduce pressures, trial full cuff deflation on vent, assessing laryngeal function. Speech continues.
Continue to wean off vent, allowing speech and swallowing
OUTCOME - combined respiratory and laryngeal wean allows speech and encourages swallowing as well as respiratory function Figure 1- Laryngeal wean process
References & acknowledgements 1.Leelapattana P, Fleming JC, Gurr KR et al. Predicting the need for tracheostomy in patients with cervical spinal cord injury. J Trauma Acute Care Surg. 2012; 73: (880-4). 2.Shem K, Castillo K, Wong S et al. Dysphagia in individuals with tetraplegia: incidence and risk factors. J Spinal Cord Med. 2011; 34: (85-92). 3. Altman KW, Yu GP, Schaefer SD. Consequence of dysphagia in the hospitalized patient: impact on prognosis and hospital resources. Arch Otolaryngol Head Neck Surg 2010;136(8):784-9 4. Spinal Injuries Association. A Paralysed System? (2015) Available from: http:// www.spinal.co.uk/userfiles/images/uploaded/pdf/382-783205.pdf Accessed 4th August 2015 5.Respiratory Information for Spinal Cord Injury. Weaning Guidelines for Spinal Cord Injury Patients in Critical Care Units (2012) Available from: http://www.risci.org.uk/NSCISB%20RISCI %20final.doc Accessed 4th August 2015 Thank-you to colleagues at the London Spinal Cord Injury Centre. Patient consent was gained.
Increasing self-‐ven5la5on with expiratory airflow into upper airway
• Weekly specialist multi-disciplinary tracheostomy team ward round to plan and monitor weaning programmes 5.
Tracheostomy + 24 hour ven3la3on Tracheostomy wean – cuff defla3on on ven3lator Tracheostomy wean – cuff defla3on OFF ven3lator < 30 minutes Tracheostomy wean – cuff defla3on OFF ven3lator < 30 minutes Tracheostomy wean – cuff defla3on OFF ven3lator > 60 minutes Tracheostomy wean – ven3lator free ≥12 hours Tracheostomy wean – ven3lator free ≥24 hours
Scale of swallowing ability
On discharge FEES Level 1 (+ 4 months)
3 4
5
6 7
Informal scale of weaning
Modified from Crary et al, 2005
Secre3on Ra3ng (Murray)
1 2
PAS Score
Swallow outcome Ven3la3on/ Tracheostomy status
Thin fluids-‐7 SoO solids -‐3
SoO/normal diet. 3x meals per day. Self feeding with set-‐up & assistance
Route of nutri3on Method of communica3on
Self ven5la5ng Oral diet. Fluids during the day (12 only via PEG. hours). Size 8 Bivona TTS. Cuff deflated with Passy Muir speaking valve; cuff par5ally inflated overnight. Forced vital capacity 1.18 litres
Verbal communica5on. Moderate dysarthria, intelligible to familiar listener
Discussion: • This single case study demonstrates the benefits of multi-speciality input in the management of complex conditions. Significant positive outcomes were possible for speech, swallowing and respiratory function, despite the time since injury. • The subtle presentation of dysphagia demands accurate screening and diagnostic assessment using FEES. • Early FEES supports effective weaning and swallow rehabilitation, preventing pulmonary complications & provides patient biofeedback. • CSCI patients benefit from a structured respiratory weaning plan and daily intensive & targeted swallow therapy, which combines both motor and sensory components of swallow function. • Engaging laryngeal function early through cuff deflation improves cough, secretion managements and allows speech for communication. Safe restoration of oral intake and speech is possible in CSCI, even those who are ventilator dependent and with chronic dysphagia.