been built on Dr. Richard Clarke Cabot's dictum: "The job of the physician as physician and teacher is not just to tell but to convince." The operative words in this ...
Canad. Med. Ass. .*
JASON:
April 3, 1965, vol. 92
outcome will do. If a trainee emerges knowing something more about the way others learn, with a somewhat greater skill in the use of instructional tools, an enhanced competence in developing or selecting or employing evaluation methods appropriate to his educational goals, some familiarity with the means of curriculum construction, but most important with a sense of humility about his own knowledge of educational process and a readiness to learn more from the sources so readily available, then we should not be discouraged or
PROGRAMMED INSThUCTION
711
disappointed. In a nation which talks glibly of puffing a man on the moon this may seem a paltry goal, but it is comforting to recall the wisdom of the Chinese sage who noted that "the journey of ten thousand miles begins with a single step." Until now we have been reluctant to take that step in medical teacher training, even while bemoaning failure to achieve the final destination. There will never be a better time to put aside the indecision-or arrogance-of the past, and begin the work that must be done.
Programmed Instruction: New Bottle for Rediscovered Wine HILLIARD JASON, M.D., Ed.D.,* Roche&ter, New York, U.S.A.
ABSTRACT Programmed instruction is attracting attention at all educational levels. While this approach is new, the educational principles it incorporates are well established: instructional goals are defined in advance, the content is meticulously organized, active student participation is demanded, immediate feedback is provided to students, and each instructional unit is subjected to testing and revision. With its established effectiveness as a vehicle for introducing new topics, and for providing remedial and supplementary instruction, it can free the medical teacher to devote his time to matters which are more deserving of his attention, such as identifying and responding to individual student needs, exploring complex concepts, and working directly with students to provide a model and critical supervision. A more important potential contribution of programming may be that it has reminded us of sound educational precepts which deserve our attention in all forms of instruction.
I N THE minds of some, the term "programming" stirs associations to electronic computers and the term "teaching machine" suggests automation, both tending to create images of dehumanized technology desecrating the sacred ground of the student-teacher relationship. In point of fact, the analogy to computers is apt, but for quite another reason. Programming a computer requires meticu*Associate in Medical Education and Assistant Professor of Psychiatry, School of Medicine and Dentistry, University of Rochester.
SOMMAIRE A tous les niveaux, l'enseignement programm. attire l'attention des corps enseignants. Bien que ce mode d'instruction soit nouveau dans son application, ses principes de base sont bien connus: les buts . atteindre sont formul6s d'avance, la mati.re est m6ticuleusement pr6par6e, la participation active des 6tudiants est indispensable et exig6e, un moyen de contr6le et de correction 6ventuelle du travail de l'6tudiant est pr6vu et le rendement de chaque "unit6" d'enseignement est soumis . l'analyse critique et . une r6vision 6ventuelle. Cette m6thode, grAce ii son efficacit6 ind6niable pour introduke de nouveaux sujets, pour completer l'enseignement et rem6dier . ses insuffisances, permet au professeur medical de consacrer son temps A des tAches plus dignes d'attention, parmi lesquelles on peut signaler: d6couvrfr les faiblesses individuelles de l'.tudiant et y parer, analyser des principes complexes et travailler directement avec l'6tudiant, ce qui assure une surveillance critique mod.le. La programmation, outres ses m6rites intrins.ques, a peut-.tre une cons6quence plus importante, celle de nous rappeler les sains principes de l'enseignement qui m6ritent d'.tre retenus dans tous les domaines de l'instruction.
bus preparation, precise organization, flawless ap. plication of procedure and repeated testing to assure that the task has been accomplished with maximum effectiveness. A basic premise of programmed instruction is that a similarly stringent approach can be applied to the task of helping people learn.
712
JASON:
PROGRAMMED INSThUCTION
It was Skinner's1 co iction that we know far more about teaching and learning than gets applied in the classroom, a conviction which led to his now classic paper1 'and the subsequent development of programmed instruction. Throughout this past half century a variety of theoretical positions 'and much experimental evidence have accumulated, materially enhancing our understandings of how people learn. While much controversy remains, there are several key issues that can be considered resolved. It is these fundamental principles of learning which can be translated into specific operations required for effective teaching. Programmed instruction is the first educational technique to incorporate these principles systematically. PRINCIPLES OF LEARNING A.ND TEACHING
Those propositions about human learning which can now be considered established, and the guidelines for teaching which follow, can best be described as responses to questions that all teachers should ask themselves when planning a course of instruction. Individually, these questions may appear 'as banalities; collectively they make the difference between a random, intuitive effort and professional, effective teaching. What should the students learn? Before embarking upon any instructional endeavour, however brief or extended, each teacher must determine the specific "content" of his unit of instruction. Indeed, he will do well to classify the content in terms of its characteristics: whether it consists of: (a) straight information, (b) the understanding of interrelationships among segments of knowledge, (c) the application of these understandings to new situations, (d) the capacity to accumulate and assess new information, (e) the performance of certain intellectual, sensory or manual skills, or some combination of these. The teacher, in fact, may determine that the content of his instruction should include learning of still another kind: he may consider that a serious intent of his instruction is the modffication of certain "non-cognitive" characteriStics of his students; whether it be 'the enhancement of their sense of responsibility to patients, the promotion of positive attitudes toward a particular approach to medical practice or an improvement in their capacity to remain sufficiently detached to be clear-headed while being kind and supportive. * What will be considered satisfactory performance? Beyond determining the specific content' of a course of instruction, the teacher must decide how much of each aspect of this content a student must acquire to be considered as having fulfilled the aims of the course. While it is far easier to *Two very useful references for the precise delineation of instructional objectives are the handbooks edited by Bloom2 and Krathwohl et al.3
Canad. Med. Ass. 3. April 3, 1965, vol. 92
decide simply that whatever, say, the best 80% of the class can do will be regarded as sufficient, there is no justification for such an approach. In the small-size student groups with which we deal there is no rational basis for a priori decisions re.. garding the relative distribution of talent. Good teaching should generally enable virtually all to succeed. For effective teaching it is both possible and necessary to establish, in advance, the minimum standards of acceptable performance.* What will each student have to do to demonstrate that he has achieved the expected level? Having defined the goals of the educational program and the minimal level of achievement expected, the teacher should specify, in advance, those behaviours he will look for in his students to assure that the intended learning has indeed occurred. The teacher must decide, for example, whether 'the goals of his instruction will have been fulfilled when a student can describe the physical findings which differentiate among the various valvular diseases of the heart, or whether his real intent is to help students actually develop the capacity to s'ystematieally examine and diagnose patients with heart lesions. Performing at some acceptable standard of "describing" can give no assurance of capacity to negotiate satisfactorily the examination and diagnosis of a patient. If it is indeed the second that is intended, this must form the basis for both teaching and testing. Similarly, all of an instructor's objectives should be formulated in terms of the operations or behaviours to be performed by the students.t What are the characteristics of the students for whom the instruction is intended? In the simplest of terms, there is not much point in offering a course of instruction for a group of 'students who are all beyond the level of accomplishment that the instructor intends them to achieve. Any instructional planning must take into account a precise knowledge of the background, strengths and limitations of the students involved. Unless the teacher and his student have very similar poin'ts of departure, they will have difficulty finding a common path to follow on their way to their supposedly mutual goal. How can the students best be led from their own starting paints to the stated goals? This is an enormously complex question with no simple answers. The specific instructional techniques selected by the 'teacher must depend heavily upon his own experiences, characteristics 'and intentions. The choice of techniques must depend, also, on the goals to be achieved. There are, however, several guidelines that transcend specific 'techniques and have relevance for all instructional endeavours. A helpful reference for defining the goals of any educational effort, whether small or large, is the report edited by LindvalL4 tMager5 has written an excellent, brief, programmed text on the designing of instructional objectives in behavioural terms.
Canad. Med. Ass. J. April 3, 1965, vol. 92
JASON:
BEGIN HERE
.
p
Do no look at answer (direr ily below) until..ou have compl eted Frame I.
1
4 see answer
PROGRAMMED INSThUCTION
713
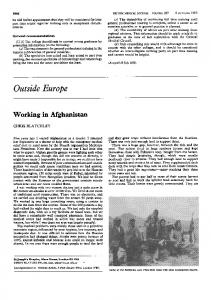
The diagram below, taken from the Lead I tracing of a normal subject, shows the standard deflections of the electrocardiogram.
Label the five deflections, using the conventional letters P, Q, R, 5, and T: Circle the QRS complex. The T wave is El positive El negative
o.b
'1
h.7 I
2 The Q, R, and S waves are defined as follows: The Q wave is the negative (downward) deflection which initiates the QRS complex. The R wave is the positive (upward) deflection of the QRS complex. The S wave is the negative deflection immediately following the R wave.
In each QRS complex below, label the Q, R, and S waves if they are present:
positive
a+
2
a+bL
V
I
A Q wave wider than one standard division, i.e., longer than 0.04 second in duration, is considered abnormal. Under each diagram, indicate whether the Q wave is normal or abnormal:
I*1
I
a
b
-'
d
e
Fig. 1.-Brief sample from a linear program. (Reproduced by permission from Spectrum, September-October 1962.)
These guidelines are derived from the following propositions: 1. Effective learning requires the active participation of the student. The more the student "does", i.e. the more of his faculties he brings to bear upon the learning task, the more effectively will he learn. Effective teaching, therefore, must demand something of the student; it can't simply tell the student what he should know. 2. Demands that are made upon students, the challenges to which they are subjected, must fall within their "learning range"-that is, not too easy and not too difficult. 3. Effective learning requires constant feedback. It is equally important to be informed that one is proceeding correctly as it is to discover that an incorrect path is being pursued. In fact, it is a human characteristic that being informed that one is correct serves as a reward", and tends to reinforce learning.
4. Humans have a very limited capacity for learning isolated facts. For information to be of any use it must be understood in terms of the organizing principles to which it applies. Effective teaching requires that the basic principles of a discipline be clearly identffied and developed in the sequence which experimental trial shows that students actually follow. Has the instructional unit achieved its purposes? The fact of the teacher's having undertaken a course of instruction is no assurance that his students have learned. The teacher who has defined his goals in advance, and specified the outcomes expected in the students, can determine with considerable precision how much learning has occurred. If, as generally happens, the learning has been something less than perfect, he has yet to determine whether the limitations are inherent in the students or in the instructional program. There are now techniques available by which he can care-
714
JASON:
Canad. Med. Ass. 3. April 3, 1965, voL 92
PROGRAMMED INSThUCrION
fully analyze both his teaching and testing procedures, identify areas where improvement is required, undertake the necessary revision, and try again. To date, programmed instruction has been the only educational approach which, by definition, has insisted that all the steps defined by the foregoing questions be followed as inherent parts of the plan and design of teaching. Tmi Cim.n.c-ri.msncs OF PROGRAMMED INSTRUCrION
"Programmed instruction" has come to mean those materials which are designed according to the principles cited above and which are intended for individualized consumption by students. Most programs are characterized by discrete steps which build sequentially, leading the student through increasing levels of accomplishment, in terms of the objectives of the specffic unit. At each step, the student is expected to formulate a response to a specific question. If he is correct, he receives immediate confirmation (feedback) and moves on. If he responds incorrectly, he learns of his error and can review before continuing. Many styles of program sequencing and modalities for presentation have been developed. For this introduction, *the two basic sequencing approaches (linear" and "branching") and the two most common presentation formats ("text" and "machine") will be discussed. * Linear and Branching Programs A programmed unit which carries all students along the identical path, proceeding uninterruptedly from one step to the next, is aptly described as "linear". A brief segment of a linear program is presented in Fig. 1; this is schematically described in Fig. 2.
A.D.A-.LhAKIi.A Fig. 2-Schematic segment of a linear program. (E = Frame. . = Response.)
Branching programs provide for a variety of possible sequences. While styles vary considerably, all branching programs will, in some measure, lead the student along an individualized path, according to his responses to key questions. One approach provides multiple-choice questions with each instructional step (frame). If the correct response is provided, the student is instructed to proceed to the next frame. If one of the incorrect choices is made, the student is referred to one or more frames which provide appropriate "remedial" instruction. In some branching programs, quesFor a comprehensive introduction to the full field of programmed Instruction, see Lysaught and Williams.6
tions are interspersed which are designed to detect an advanced level of 'learning. In this manner, a student can be identified for whom portions of the regular program would be superfluous. They are directed to frames that are further along, thereby skipping the unnecessary section. A sample segment from a branching program is schematically presented in Fig. 3.
F - - - - -
Li]A -.
-- -g
-> Li] -.A. Li»..
Fig. 3.-Schematic segment ([1 = Frame. A = Response.)
of a branching
program.
Text and Machine Programs All programs which are presented through the modality of the printed page are referred to as "texts". For linear programs, the student follows the pages in sequence, as he would with a conventional book. He will, however, find some device to assist him in concealing the correct responses to each frame's questions until he is ready to view them. This is often accomplished by placing these answers with the next frame on the succeeding page. Since less than a full page is required per frame, only, say, the upper third of the page will be used on the first trip through the text. After completion of the top frame of the last page, the student returns to the second frame on the first page, and proceeds through the text again. Texts for branching programs are far less orderly. Indeed, they are generally called "scrambled books". The student is guided through his individualized sequence by being referred to the page number or the frame number where the next step he is to take will be found. He, therefore, is constantly leafing back and forth through the text, following the sequence which is most adapted to his pace. Teaching machines are mechanical devices for presenting the same material that forms the substance, of programmed texts. These contrivances range from simple gadgets which function as mechanical page-turners to fairly complex electronic equipment. The latter "machines" are designed for presentation of elaborate branching programs which have been placed on specially notched ifim. Each multiple-choice question is answered by pressing a lettered button, corresponding to the choice being made. The film notches provide a code which directs the electronic circuitry to move the film to the next appropriate frame; whether for remedial instruction, review,
Canad. Med. Ass. J. April 3, 1965, vol. 92
sequential advancement, or accelerated advancement to a new segment, according to the characteristics of the student's response. SOME IMPLICATIONS FOR MEDICAL EDUCATION
Programmed instruction, fundamentally, is a technology. It is a particularly distinguished educational technique because it is the first to incorporate established learning principles regularly, the first to be subjected to careful testing and evaluation and the first that can be said to have been demonstrated as an efficient and effective avenue to learning. Several current conditions in medical education combine to create a genuine need for just such an approach: 1. The growth of medical knowledge demands that educational practices be constantly re-exammed to assure that they are as efficient and effective as possible. The limited curricular time available must be used in the most satisfactory manner available. 2. Medical schools are responding to the increasing need for physicians by enlarging their class size. This requires that educational programs be designed to provide for iDdividual differences among students and to assure the continuation of the close student-faculty relationships that pertain with smaller classes. 3. The persistent shortages of faculty time for teaching require that their efforts be exerted in those areas for which they can make unique contributions. All areas that can be served equally well or better by other instructional modalities should be identffied, developed and refined. 4. It is now recognized that the pattern of lifelong study needed by physicians is best developed in school, where assistance can be provided in the acquisition of both the skills and attitudes required for effective self-instruction. Research, to date, suggests that programming can have important implications for the student, the instructor, and the overall curriculum. It makes provision for the many 'individual differences among medical students, it demands their active participation, provides them with both the knowledge and satisfaction that progress is being made, and informs them accurately, in advance, of the teacher's instructional intent. Blyth7 has eloquently pointed out that the instructor who uses programs to help students master the introductory (often prosaic) aspects of his topic, finds that he can then devote his meetings with them to the more rewarding tasks of exploring advanced concepts and of generally dealing with "higher" cognitive goals. The teacher who has engaged in actually programming a unit often finds himself a better instructor as a consequence. The contingencies of designing a program demand the application of sound educational principles. The experience of having once applied and witnessed
JASON:
PROGRAMMED INSThTJCTION
715
the results of those approaches is a most effective learning experience for teachers. It is painfully obvious that in any endeavour one can neither steer a path nor determine that one has arrived at completion without a clear, advanced notion of the desired destination. Yet, in medical education our goals have been so illdefined and fluctuating that 'there can be little wonder at the disturbing variability in quality found when medical practice is critically examined.8-'0 Possibly most disconcerting is the lack of relationship between quality of practice and the medical school grades these physicians had received. It appears that the medical school faculties were teaching or testing for material which differed from that required in practice. It is very unlikely that such was their intent. Most probably, this was the consequence of a failure to formulate goals adequately. The strict insistence of programmers on the need for well-defined objectives can only have a salutary effect on the curriculum at large. Increased attention to defining the specific intent of the overall effort and of the individual units of instruction will lead to the reorganizing of curricula on a basis which is far more meaningful than the "squatters-right" mechanism which is still so common. CoNclusIoNs
Many medical instructors have inquired if programmed instruction can replace teachers or make their jobs easier? The reply to both questions is an emphatic "No!" 'Programmed units have indeed been demonstrated to do as well as or better than some of those things which teachers now do. The attraction of programming is that it can free the teacher to do those things which he alone can do, and which are far more deserving of his attention. Attending to these cther matters, however, presents the teacher with a greater challenge. Preparing a formal presentation 'of a body of information demands less effort and skill than are required for helping students to deal with intangibles, for assisting their development of problemsolving skills or for enhancing those personal characteristics like responsibility and dedication which make such a difference in their quality as physicians. It was 'fully 50 years ago when Thorndike" wrote, "A human being should not be wasted in doing what forty sheets of paper or two phonographs can do. Just because personal teaching is precious an'd can do what books and apparatus cannot, it should be saved for its peculiar work. The best teacher uses books and appliances as well as his own insight, sympathy and magnetism." Medical teachers have begun to use programs in imaginative ways. Chnstensen'2 sends a short unit on "pH and Dissociation" to the accepted candidates at the University of Michigan, School of Medicine. The students work with this pro-
716
JASON:
PROGRAMMED INSThUCTION
gram at *their leisure during the summer prior to medical school, and the course in biochemistry can now be organized at a more advanced level than ever before. Many other instructors are using programs to help selected students overcome specific deficiencies, to pursue special interests, or to review particular material. Programming does clearly seem to be an attractive educational approach, but it must be recognized as being primarily a form of packaging which derives its strength from the established principles it contains. It does nct have exclusive rights to these contents. In fact, its greatest service may ultimately be that it has so effectively reminded us that these principles are sound and that when they are correctly applied, they work. Those of us who have responsibility for the quality of the educational experiences of our future physicians would seem obliged to look very closely at the potential contribution to be derived from both the new technique of programmed instruction and the precepts which are its substance.
Canad. 1965,Ass. vol. J.92 April 3, Med.
to repeated testing and modification, the developers of programmed instruction have provided us with an approach which holds promise for assisting with the solution of several current problems in medical education. Of greatest importance, this approach: (1) may help free the teacher to devote himself to those tasks for which he is best suited and (2) may contribute to the general elevation of instractional quality through its "rediscovery" of precepts which should guide all of our educational endeavours.
For some years we have known, but generally failed to apply in our teaching, a group of fundamental principles of learning. By incorporating the features of: precisely defining objectives in advance, meticulously organizing and sequencing the content, demanding active student participation, providing immediate feedback on pefformance, and by adopting the "experimental approach" of subjecting this technique
REFERENCES 1. SKINNER, B. F.: Harvard Educational Review, 24: 86, 1954. 2. BLOOM, B. S., editor: Taxonomy of educational objectives; the classification of educational goals, handbook one, the cognitive domain, Longmans, Green, Co., Inc., New York, 1956. 3. KRATHWOHL, D. R. et aL: Taxonomy of educational objectives, the classification of educational goals, handbook two, affective domain, David McKay Co. Inc., New York, 1964. 4. LINDYALL, C. M., editor: Defining educational objectives, the University of Pittsburgh Press, Pittsburgh, Pa.. 1964. 5. MAGER, R. F.: Preparing objectives for programmed Instruction, Fearon Publishers, San Francisco, Calif., 1961. 6. LYsAUGHT, 3. P. AND WILLIAMS, C. M.: A guide to programmed instruction, John Wiley and Sons, Inc., New York, 1963. 7. BLYTH, 3. W.: Teaching machines and human beings. In: Teaching machines and programmed learning; a source book, edited by A. A. Lumsdaine and R. Glaser, National Education Association of the United States, Washington, D.C., 1960, p. 401. 8. PETERsON, 0. L. et al.: .T. Med. Educ., 31: 1, No. 12, (Part 2), December, 1956. 9. CLUTE, K. F.: The general practitioner, The University of Toronto Press, Toronto, 1963. 10. PRICE, P. B. et al.: ,T. Med. Educ., 39: 203, 1964. 11. THORNDIKE, E. L.: Education, a first book, The Macmillan Co., New York, 1912, p. 167. 12. CHRISTENSEN, H. N.: The identification of special topics for teaching by short "plug-in" programs. In: Programmed instruction in medical education, Proceedings of the Rochester Conference, edited by 3. P. Lysaught, The University of Rochester, to be published.
THE CONVINCER No two physicians perform their educational services alike and tomes have been written by advocates of various methodologies. In considering this problem with senior medical students, who in a year will be teaching medical students how to inform patients, a useful discussion has been built on Dr. Richard Clarke Cabot's dictum: "The job of the physician as physician and teacher is not just to tell but to convince." The operative words in this golden maxim are "teacher" and "convince". One can only guess at the many hours the clinician spends educating his patients as the latter strive to adapt to the handicaps of diabetes mellitus or to achieve rehabilitation after damage to the spinal cord. 'In preparing for this pedagogic endeavor, the senior student has two choices. Should he adopt the easy, less time-consuming but less effective, laissez-faire or "telling" method in communicating with his patients, their families and his, future students; or should he practice the more difficult "convincing" method which draws its life from detailed, repetitive presentations, responsiveness to questions, and, above all, an appeal to the self-interest of the patient, family, or student? Barring language difficulties, low intelligence, or cussedness, the failure of a patient to follow his doctor's instructions is usually due to the physician's subconscious or conscious acceptance of the role of "teller" rather than convincer The senior medical student should be urged to see in his daily clinical work not only the immediate medical problem but also the opportunity to test the relative value of the "tell" and "convince" methods of communicating with patients and their families. When case presentations are evaluated during preceptoral meetings, it is useful to place the student in the role of
gentle critic of remarks by his peers. After he appraises a case history by one of his fellows, he may 'be asked how he would characterize a good history to his future students. Such a discussion usually presents the opportunity to emphasize the factor of self-interest in the educative process. The medical student has a better understanding of the educational continuum when he is oonvinced that the history he constructs is his signature and professional image to his colleagues. He learns that the history is a living document and not some inert words on paper to be added to the reams of dusty files in the record room. He becomes aware that in making the effort to produce an accurate account of the interaction between the patient and his disease, he is advancing his clinicianship not only with respect to the illness immediately at hand but also to coexisting problems which sometimes prove more self-educative and important to the patient 'than the obvious presenting disorder. A satisfying conclusion arises when the student learns to define a good history as one which taken by "Dr. A" can be used effectively by "Dr. B", and vice versa. This approach often pacffies the angry or disappointed student who has been asked to revise his history several times. The thinly suppressed growl or grimace at the instructor who has only told him that the history is inadequate is replaced by compliance and a better performance if the preceptor convinces the student that the test of a good history is that it should meet the requirements of the next good doctor. Peace then reigns. Of equal importance, however, is the student's learning a technique which he may find useful when he assumes responsibility for a similar teaching exercise in the future.-D. Seegall, I. Med. Educ., 39: 1032, 1964.
SUMMARY