562
Medical Informatics in a United and Healthy Europe K.-P. Adlassnig et al. (Eds.) IOS Press, 2009 © 2009 European Federation for Medical Informatics. All rights reserved. doi:10.3233/978-1-60750-044-5-562
Feasibility Study of a Web Application for Self-Report of Anticancer Treatment Toxicities Vincenzo DELLA MEA a,1 , Ivan DE MOMI a, Giuseppe APRILE b, Fabio PUGLISI b, Jessica MENIS a, Anica CASETTA c, Silvia BOLZONELLO b, Gianpiero FASOLA b a Department of Mathematics and Computer Science, University of Udine, Italy b Department of Oncology, University Hospital of Udine, Italy c Department of Epidemiology, University of Udine, Italy
Abstract. Collection of collateral effects related to toxicities suffered by patients being exposed to anticancer treatments is of crucial importance in clinical practice but also in oncological research. The present paper describes a web application called PaTOS for self-report of anticancer therapy toxicities, and its evaluation in a preliminary interface analysis and then in a feasibility study. Keywords. Web 2.0 applications, home-based eHealth
1. Introduction Collection of collateral effects related to toxicities suffered by patients being exposed to anticancer treatments is of crucial importance in clinical practice but also in oncological research. The usual way of recording such symptoms is by means of a doctor-patient dialogue carried out during the pre-therapy visit. However, discrepancies outcropped when traditional modalities in collecting information regarding toxicities suffered by patients being exposed to anticancer treatments have been compared to direct selfreports [1]. Reasons for such differences are due to the whole chain intercurring between patient experience of the symptom and recorded data usage [2]: clinician interpretation of symptom during interview, written representation of symptom, eventually further interpretation of written symptom by a research assistant and its translation as data written in some research database are all steps that might be subject to error. The basic idea underlying the approach discussed in the present paper is to shorten that data coding chain, to reduce possible error sources during data registration. This means giving the patient some more responsibility and power in reporting his/her symptoms, according to those principles recently called “Medicine 2.0” [3] after the name “Web 2.0”. One way of interpreting such principles into the online healthcare framework is that of a larger consumer involvement into production and registration of health data 1 Corresponding Author: Vincenzo Della Mea, Department of Mathematics and Computer Science, University of Udine, via delle Scienze 206, 33100 Udine, Italy; E-mail:
[email protected].
V. Della Mea et al. / Web Application for Self-Report of Anticancer Treatment Toxicities
563
regarding him/herself. Access to their own data has been recognised as useful since eighties [4], and more recently Internet health records have been indicated as a technical facilitators for that [5]. In fact, after pioneeristic experiences of some years ago [6–9], some commercial proposal is now gaining momentum, like Google Health and Microsoft HealthVault, that gives consumers a way for recording their health data and then giving online access to healthcare professionals. Starting from these principles, we hypothesized that a Web 2.0 application could be an accurate and reliable tool to directly record toxicity data by the patient, to help in reducing recording and interpretation errors. Some previous experience is available in other clinical fields that supports this kind of application: in diabetes management [10], asthma monitoring [11], heart failure [12]. In oncology, a notable experience has been made by Basch et al. [2] that also suggested attention to reminders and clinician feedback. The present paper describes a web application called PaTOS for self-report of anticancer therapy toxicities, and its evaluation in a preliminary interface analysis and then in a feasibility study.
2. Methods 2.1. Data Collection In the analysis phase conducted with joint meetings between computer science experts and oncologists a number of specifications have been developed that included also a specification of the data to be collected. Patients were supposed to provide selfcollected data at least once a week, with the possibility to contribute more than one time a week if they wanted to. Symptoms were to be reported day by day, if any. To code symptoms, it has been decided that a simplified, patient-adapted definition of type and NCI-CTCAE grade [13] of the 15 commonest toxicities has to be used, together with the possibility of reporting previously undefined symptoms by means of a free text area. Patients had control visits every two weeks, where they reported symptoms in the traditional way, for comparison with self-registered ones. 2.2. The Web Application To support data collection, a web application called PaTOS has been developed using Java 2 Enterprise Edition and MySQL as a database server that fulfills specifications coming from domain experts. Using PaTOS through home Web access, each patient can access using a personal username and password and compile a daily report of the affecting toxicities by choosing and grading any of them from the user interface. If too much time has passed since the last patient report, PaTOS will send the doctors a communication about the missing data. This decision also takes into account suggestions about reminders and clinician feedback discussed in [2]. Physicians access to a specific part of the site where they can perform managing operations on patients’ data, as inserting or updating database information and visualize flowsheets of patient toxicities by means of graphing functions.
564
V. Della Mea et al. / Web Application for Self-Report of Anticancer Treatment Toxicities
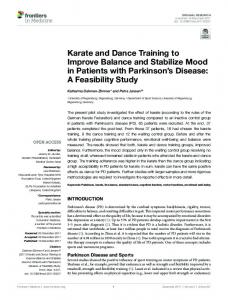
To help in application evaluation, a log subsystem has been implemented to record every action carried out by users. To verify the usability of the developed application, a first preliminary test aimed at interface analysis has been carried out before adopting it in a real world feasibility study. PaTOS usability test involved 8 non patient users, chosen among people with oncology knowledge, to which two simulated toxicity scenarios have been proposed for coding into the system [14]. This first test allowed to recognise some minor misbehaviour in the interface, mainly related to unclear day selection, that lead to a redesign of some parts of the application, together with a general esthetical enhancement to make it more user friendly. After that, the application has been considered ready for a feasibility study on oncological patients. Figure 1 shows two snapshots of the application.
Figure 1. Two PaTOS snapshots
For the first test and feasibility study the approach to privacy and security issues has been simplified: no personal data are inserted into the system, and the patient accesses the application by means of an anonymous code that is related to his/her data only on an independent archive (actually, paper-based). 2.3. Subjects Eligible patient were consecutively chosen among those starting an antitumoral treatment in the Department of Oncology of the University Hospital of Udine, Italy. Of 56 contacted patients, 30 accepted and signed an informed consent. Patients were representative of various tumoral diseases.
3. Results 28 out of 30 patients were observed during 10 weeks, corresponding to one (8 patients) or two (20 patients) completed treatment cycles.
V. Della Mea et al. / Web Application for Self-Report of Anticancer Treatment Toxicities
565
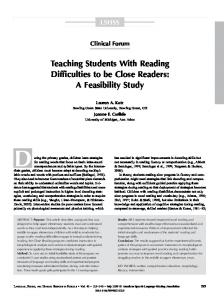
In the observation period, users did a total of 231 accesses, plus a number of failed access attempts (due mainly to wrong password). 193 accesses were fully completed, resulting in the registration of symptoms. Among the uncompleted accesses, some were due to a missed final step in registration, caused by a click towards password modification. Apart from some minor pitfall, the web application appeared surprisingly quick to learn and use. Figure 2 shows a graph of average time per patient, adjusted per number of symptoms reported. Learning time was also evaluated: between the first and sixth input session, time decreased of about 50% on average.
Figure 2. Adjusted average input time in minutes per patient
Only 18 out of 193 input sessions were reported to be carried out by family instead that directly by the patient. At the end of study time, patients inserted a total of 1,870 symptoms observations (average: 69 per patient, 1.5 per day). Self-reported data were compared with data registered during control visits by means of K-statistics. Although the statistical method revealed not fully adequate due to the large amount of symptoms non graded, comparison revealed a greater precision in reporting at home than during the visit, possibly due to the almost realtime registration after episodes, and in particular for low intensity symptoms, which are easier to forget, although they help oncologists to better personalize treatment. Of 1,870 observations, 851 were related to toxicities of degree 1, 652 of degree 2, 254 of degree 3. The free text box available at the end of the questionnaire has been used 44 times, only two for a toxicity not present in the list, the other for communications to the oncologist. Self-reported symptoms distribution was compatible with frequencies reported in literature. In fact, the most selected toxicity was tiredness (408 observations, 22% of total), the least one was fever (13 observations, 0.7% of total).
4. Discussion While only a prototype, the proposed system appeared to be a good way to collect anticancer therapy toxicity information directly by the patient, overcoming problems
566
V. Della Mea et al. / Web Application for Self-Report of Anticancer Treatment Toxicities
related to memory, which usually makes low degree symptoms be unreported to the oncologist. Agreement between self-reported data and data communicated to the oncologist was good for the most objective observations, less for observations where doctor and patient perceptions may differ. Time needed for input was lower than expected, with about 6 minutes per session on average. Not all patients complied with the request for at least one input session a week, although some of them accessed the system more often, possibly during or after symptoms. Although the sample involved in this feasibility study was small, the results have been convincing, and now a clinical trial is starting, with a larger user base. At the same time, a technical solution is being studied to embed the system into the regional citizen portal that provides secure access authenticated by means of a smart card. On the physician side, currently an oncologic patient record exists where doctors record toxicities, but that is not yet linked to the PaTOS application. After a more formal clinical trial however PaTOS will be connected to the patient record to avoid data entry duplication.
References [1] [2]
[3] [4]
[5] [6]
[7]
[8]
[9] [10] [11] [12]
[13]
[14]
Cella, J.A., Hays R.D. (2005) Clinical significance of patient-reported questionnaire data: another step toward consensus. Journal of Clinical Epidemiology 58(12):1217–1219. Iasonos, A., Barz, A., Culkin, A., Kris, M.G., Artz, D., Fearn, P., Speakman, J., Farquhar, R., Scher, H.I., McCabe, M., Schrag, D. (2007) Long-term toxicity monitoring via electronic patient-reported outcomes in patients receiving chemotherapy. Journal of Clinical Oncology 25(34):5374–5380. Eysenbach, G. (2008) Medicine 2.0: Social Networking, Collaboration, Participation, Apomediation, and Openness. Journal of Medical Internet Research 10(3):e22. Baldry, M., Cheal, C., Fisher, B., Gillett, M., Huet, V. (1986) Giving patients their own records in general practice: Experience of patients and staff. British Medical Journal (Clinical Research Ed.) 292(6520):596–598. Eysenbach, G., Jadad, A.R. (2001) Evidence-based patient choice and consumer health informatics in the internet age. Journal of Medical Internet Research 3(2):e19. Cimino, J.J., Patel, V.L., Kushniruk, A.W. (2002) The patient clinical information system (PatCIS): technical solutions for and experience with giving patients access to their electronic medical records. International Journal of Medical Informatics 68(1-3):113–127. Masys, D., Baker, D., Butros, A., Cowles, K.E. (2002) Giving patients access to their medical records via the internet: the PCASSO experience. Journal of the American Medical Informatics Association 9(2):181–191. Hassol, A., Walker, J.M., Kidder, D., Rokita, K., Young, D., Pierdon, S., Deitz, D., Kuck, S., Ortiz, E. (2004) Patient experiences and attitudes about access to a patient electronic health care record and linked web messaging. Journal of the American Medical Informatics Association 11(6):505–513. Rind, D.M., Kim, J.H., Sturges, E.A. (1999) SeniorMed: Connecting patients to their medication records. AMIA Annual Symposium Proceedings 1999 1-2:1147. Armstrong, N., Powell, J. (2008) Preliminary test of an Internet-based diabetes self-management tool. Journal of Telemedicine and Telecare 14:114–116. Finkelstein, J., Hripcsak, G., Cabrera, M. (1998) Telematic system for monitoring of asthma severity in patients’ homes. Studies on Health Technology and Informatics 52(Pt 1):272–276. Wu, R.C., Delgado, D., Costigan, J., MacIver, J., Ross, H. (2005) Pilot Study of an Internet PatientPhysician Communication Tool for Heart Failure Disease Management. Journal of Medical Internet Research 7(1):e8. Trotti, A., Colevas, A.D., Setser, A., et al. (2003) CTCAE v3.0: development of a comprehensive grading system for the adverse effects of cancer treatment. Seminars in Radiation Oncology 13(3):176– 181. Fasola, G., Aprile, G., Della Mea, V. et al. (2007) Development of a web-based model to track patients’ self-reported symptoms related to anticancer treatment toxicities. Journal of Clinical Oncology 2007 ASCO Annual Meeting Proceedings 25(Suppl 18):17021.