evaluated on 1,677,116 patients, collected as part of first trimester aneuploidy screening conducted between 2003 and 2011. The study population was 65% ...
Poster Session V
Clinical Ob, Epidemiology, ID, Intrapartum Fetal, Operative Ob, Med-Surg-Diseases, Ob Quality & Safety, Public & Global Health
Odds ratios (95%CIs) from the multivariable multinomial logistic regression model for maternal placenta-related syndromes
www.AJOG.org
pregnancy complications, more difficult ultrasound examinations, reduced fetal fraction of DNA leading to poorer performance of NIPT testing and the need to ensure that weight adjustment formulas used for aneuploidy screening are still applicable. The slowing of the trend in the increase in MW needs to be studied but is a positive sign for public health.
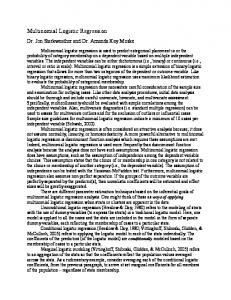
Increase in geometric mean maternal weight by year
Geometric mean adjusted for age, gestational age and ethnicity.
719 Analysis of spatial variation in prenatally diagnosed congenital anomalies in Indiana Elicia Harris1, Men-Jean Lee1, Michael Reger2, Jennifer Wessel2, Christian Litton1, Frank Schubert1, Alan Golichowski1 1 Indiana University School of Medicine, Obstetrics and Gynecology, Indianapolis, IN, 2Indiana University School of Medicine, Public Health, Indianapolis, IN
718 First trimester maternal weight in USA continues to rise Mark Evans1, Terrence Hallahan2, Hsiao-Pin Liu2, Jon Carmichael2, David Krantz2 1 Comprehensive Genetics, Genetics, New York, NY, 2Perkin Elmer, NTD Labs, Melville, NY
OBJECTIVE: To determine whether the average weight of pregnant women continues to increase between 2003 and 2011. STUDY DESIGN: First trimester maternal weight (MW) data (lb) were evaluated on 1,677,116 patients, collected as part of first trimester aneuploidy screening conducted between 2003 and 2011. The study population was 65% Caucasian, 12% Hispanic, 10% African American, 7% Asian, 3% Asian Indian and 3% other ethnic Groups. If a patient had more than one test during this time period data from one of their tests was selected at random. Geometric mean maternal weight values were adjusted for age, gestational age at time of test and ethnicity by determining the least-squares means based on ANOVA using log-transformed weight values. The adjusted geometric mean maternal weight values were then regressed against time (with standard error of the coefficients adjusted for autocorrelation and number of patients during each time period). RESULTS: Overall over the study time period, the average weight of the total population increased by 4.0% while the increase in the top 10% group was 7.3%. A majority of the increase occurred from 2003 to 2007 (3.0% and 4.7% for the total population and top 10%, respectively). Regression analysis determined that the increase was not linear but rather followed a polynomial quadratic pattern for both the overall population as well as the top 10% (P value of the quadratic term ⬍ 0.001 for both overall and top 10% of the population). CONCLUSION: The continuous increase in the mean MW particularly the top 10% is of significant concern because of increased rate of
S302
OBJECTIVE: To determine if there are geographical clustering of congenital anomalies across various zip codes, counties, and economic growth regions (agriculture vs. manufacturing industries) by Indiana. gov. STUDY DESIGN: This was a retrospective study from January 1, 2008 to January 1, 2012 of 1112 individual cases of prenatally diagnosed congenital anomalies detected on Level II ultrasound at the primary statewide perinatal referral center for pregnant women whose fetuses require Pediatric Surgery, ECMO, Pediatric Cardiology, and/or pregnancy termination. Geographic Information Systems (GIS) mapping of the affected fetuses were performed using zip codes and county of residence of the pregnant women using latitude and longitude of maternal residence during prenatal ultrasound. Population data was obtained from the Indiana State Department of Vital Statistics by zip code, county, and women of childbearing age for use as denominators for rates calculations. RESULTS: Region 5 (Indianapolis) had the highest total number of anomalous fetuses (55.8%), although only 28.15% of population resides in this region according to 2010 Census data. 4 zip codes in Indianapolis (Region 5) and 2 zip codes around South Bend (Region 2) had the highest number of anomalies. However, when geomapping the fetal anomaly rate by 100,000 population, only 1 zip code was identified as having 758 fetal anomalies per 100,000 population during this time period, while the next highest zip codes had only 165-251 anomalies per 100,000 population. When the data was geomapped by county, St. Joseph County (South Bend), once again had the highest congenital anomaly rate of 790 cases per 100,000 female population of child-bearing age (15-44 years) (Figure). CONCLUSION: There appears to be geographic clustering of prenatally diagnosed fetal anomalies in particular zip codes and counties across the state of Indiana. Further epidemiological studies are needed to correlate these clusters with environmental hazards and exposures during embryogenesis.
American Journal of Obstetrics & Gynecology Supplement to JANUARY 2013
www.AJOG.org
Clinical Ob, Epidemiology, ID, Intrapartum Fetal, Operative Ob, Med-Surg-Diseases, Ob Quality & Safety, Public & Global Health
Figure
Poster Session V
Figure
720 Changing trends in intrauterine growth
721 Impact of gestational weight gain by BMI class on cesarean delivery in nulliparous women
Nancy West1, Anne Lynch2, Jan Hart2, Anusha Streubel3, Robert McDuffie4 1
University of Colorado, Epidemiology, Aurora, CO, 2University of Colorado, Obstetrics and Gynecology, Aurora, CO, 3University of Colorado, Pediatrics, Aurora, CO, 4Kaiser Permanente Colorado, Obstetrics and Gynecology, Denver, CO
OBJECTIVE: To construct updated birthweight reference standards us-
ing a large, contemporary, and race/ethnically diverse sample in Colorado in order to: 1) provide clinicians with an updated tool for fetal growth assessment and 2) provide updated norms for determination of small- and large for gestational age (SGA and LGA). STUDY DESIGN: In this cross-sectional study, weight-for-gestational age curves for neonates were constructed from birthweight measurements of 57,826 singleton infants (48.6% female). Neonates were born between 20 and 42 weeks gestation during 1999-2010 in the Denver metropolitan area. Gestational age was based on the best obstetrical estimate, which included ultrasound examination in the majority of cases. Sex-specific and combined-sex growth charts were constructed using the 10th, 25th, 50th, 75th, and 90th percentiles. A locally-weighted regression procedure was applied to the empirical weight-for- gestational age percentiles. To investigate trends in intrauterine growth, we compared our data to the Lubchenco growth data (Lubchenco, Pediatrics, 1963), which were derived from birthweights of infants born during 1948-1961 in Denver, CO. RESULTS: The updated curves are presented in the figure. On average, male neonates weighed 3284 grams and females weighed 3181 grams. For gestational ages 24-28 weeks, contemporary neonates weighed 182 grams less than the historical neonatal population. Birthweights for gestational ages 29 and 30 weeks were similar between the two populations. For gestational ages 31-42 weeks, contemporary neonates weighed 282 grams more than the historical population. CONCLUSION: We demonstrate changes in birthweights during the past 5 decades in Colorado, including a lower mean weight at early gestational ages and a higher mean weight at later gestational ages. Use of historical growth standards will likely increase misclassification of SGA and LGA in contemporary neonates. These updated norms for intrauterine growth can facilitate monitoring of fetal growth.
Nicole Marshall1, Donna Halloran2, Judith Chung3, Jonathan Snowden1, Yvonne Cheng4, Kathryn Melsap3, Elliot Main3, William Gilbert3, Aaron Caughey1 1 Oregon Health & Science University, Obstetrics and Gynecology, Portland, OR, 2St. Louis University, Pediatrics, St. Louis, MO, 3California Maternal Quality Care Collaborative, California Maternal Data Center, Stanford, CA, 4 University of California, San Francisco, Obstetrics and Gynecology, San Francisco, CA
OBJECTIVE: The cesarean rate in the United States continues to rise, as does maternal pre-pregnancy weight. While it is clear that obese women have higher rates of cesarean, the impact of gestational weight gain on cesarean rates by body mass index (BMI) group is unclear. The objective of this study was to determine the impact of various amounts of weight gain during pregnancy on cesarean rates by BMI category. STUDY DESIGN: This is a retrospective cohort study of birth records linked to hospital discharge data for all live born singleton infants 37-41 weeks gestation born to nulliparous California residents in 2007. Maternal BMI was determined from self-reported maternal height and prepregnancy weight. The World Health Organization BMI categories were followed including underweight, normal, overweight, and obese. RESULTS: There were 171,382 births meeting study criteria. While increasing maternal BMI was significantly associated with cesarean delivery, rising gestational weight gain increased the rate of cesarean delivery within each BMI group. Normal weight women who gained over 60 lbs and overweight women who gained 40-59 lbs faced a similar rate of cesarean as obese women who gained less than 20 lbs during pregnancy (⬃35-40% in all 3 groups). Obese women who gained over 60 lbs had the highest risk of cesarean at 52.5%. CONCLUSION: Gestational weight gain is significantly associated with increased rate of cesarean in nulliparous women of all BMI categories, although the rate remains strongly associated with prepregnancy BMI. By moderating weight gain, women may be able to decrease their rate of cesarean.
Supplement to JANUARY 2013 American Journal of Obstetrics & Gynecology
S303