2012 IEEE Symposium on Industrial Electronics and Applications (ISIEA2012), September 23-26, 2012, Bandung, Indonesia
Implementation of Fuzzy C-Means Clustering for Psoriasis Assessment on Lesion Erythema Ahmad Fadzil M Hani, Esa Prakasa, Hermawan Nugroho, Vijanth S. Asirvadam Centre for Intelligent Signal and Imaging Research, Universiti Teknologi PETRONAS, Bandar Seri Iskandar, Perak, Malaysia E-mail:
[email protected] Abstract— Psoriasis is a skin disease that causes the appearance of reddish and scaly skin lesions. Lesion erythema, which refers to the inflammation (colour) of psoriasis lesion, is defined as one of Psoriasis Area and Severity Index (PASI) parameters. However, visual assessment by dermatologists is subjective and results in inter-rater variations. In this paper, an objective PASI erythema-scoring algorithm has been developed. The colour of lesion erythema was found to be dependent on the normal skin tone of the affected person. Normal skin tones are categorised into four groups (dark, brown, light brown and fair skins). A soft clustering is applied to solve the ambiguity problems at cluster boundaries. CIE L*a*b* data of lesions and their surrounding normal skin are used to calculate lesion erythema. The hue difference between lesion and normal skin corresponds to the lesion erythema. Two dedicated fuzzy c-means (FCM) algorithms are applied consecutively to classify normal skin tone and to score PASI erythema. 2,322 normal skin and 1,462 lesions samples from 204 recruited patients at Hospital Kuala Lumpur are used to build skin tone and PASI erythema score classifiers respectively. Agreement values between first and second assessments of 430 lesions for PASI erythema are determined to evaluate scoring performance. Kappa coefficients are found 0.70 for all skin tones (fair - 0.70, light brown - 0.8, brown - 0.79, and dark skin - 0.90). These agreement results show that the proposed method is reliable and objective, and thus can be used for clinical practices.
Figure 1. Plaque psoriasis lesions on upper limb, trunk, and lower limb regions
Data by the Malaysian Psoriasis Registry revealed that the percentage of plaque psoriasis in Malaysia is 80.9% [7]. Psoriasis can affect any part of skin such as head, hands, trunk, feet, nail, and skin folds [8], [9]. Periodical review of medical treatments for psoriatic patient is important, as the disease cannot be completely cured. The PASI (Psoriasis Area and Severity Index) Scoring method is the gold standard for the severity assessment [10]. Four parameters namely, area (ratio of lesion area to total body surface area), erythema (lesion redness), scaliness, and thickness are required to determine PASI score. Equation (1) is used to calculate PASI score:
PASI 0.1 E T S h h h 0.3 E T S t t t
Keywords- psoriasis, erythema assessment, Fuzzy-C-Means clustering
(1)
From Equation (1), score intervals for PASI erythema (E), thickness (T), and scaliness (S) are defined from 0 to 4 whereas the interval of PASI area (A) is from 0 to 6. These parameters are assessed at four body regions - head, upper limb, trunk, and lower limb - Subscripts h, u, t, and l are used respectively for each PASI parameter. Variable Eu for instance is used to symbolise PASI erythema score at the upper limb region.
I. INTRODUCTION Psoriasis is an incurable but treatable skin disease [1]. In psoriasis, the immune system sends incorrect signals that speed up the growth cycle of skin cells. In normal condition, skin cell will grow in ± 28 days but in psoriasis, the growth can accelerate to as fast as ± 4 days. Recent studies have shown that psoriasis can significantly affect the quality of life, with many psoriasis patients experiencing social and psychological problems with their environment [2].
Although the PASI scoring has been accepted as the gold standard for psoriasis assessment, it is not used in daily practice. PASI scoring is tedious, time-consuming and can be very subjective. The subjectivity of the scores is influenced by inter and intra-rater variation of dermatologists. Therefore, an objective method is needed that is reliable, valid and consistent for any assessment.
Psoriasis affects about 2 - 3% of world population as mentioned in [3], [4]. The published psoriasis prevalence in Malaysia by Dermatological Society of Malaysia is 3% [5]. The Dermatology Department of Hospital Kuala Lumpur registered 3,906 psoriasis patients of a total of 75,883 hospital’s patients for the years 2005-2010, giving a prevalence of 5.2% [6]. Plaque psoriasis is the commonest types of psoriasis accounting to around 80% of psoriasis cases. An example of plaque psoriasis lesions on upper limb, trunk, and lower limb regions are shown in Figure 1.
978-1-4673-3005-3/12/$31.00 ©2011 IEEE
Ah 0.2 Eu Tu Su Au At 0.4 El Tl Sl Al
In this paper, performance of the proposed method in assessing and grading PASI erythema is investigated. The method is implemented in a computerised system called αPASI. The α-PASI is developed to enable PASI scoring objectively for all PASI parameters.
331
2012 IEEE Symposium on Industrial Electronics and Applications (ISIEA2012), September 23-26, 2012, Bandung, Indonesia
II. APPROACH
hab hablesion habnormal
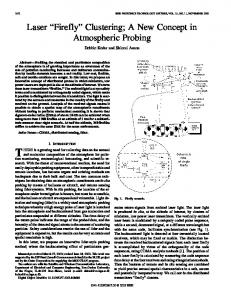
A. Computerised PASI Erythema Assessment Previous work of PASI erythema assessment has been reported [11]. To determine PASI erythema score, the skin colour (CIE L*a*b*) data of representative lesions and their surrounding normal skin are first obtained for the different body areas (head, trunk, lower and upper extremities) using a chromameter (Konica Minolta CR-400) and are analysed accordingly. Figure 2 shows the flowchart of erythema assessment of the α-PASI system.
(4)
The second stage of FCM classification method is used to classify the hue difference, Δhab values to determine PASI erythema scores. B. Kappa Coefficient for Agreement Analysis The inter-rater variation of two independent observers can be evaluated by using kappa coefficient analysis. The kappa coefficient was proposed by Cohen in 1960 and it is widely used to measure agreement among clinicians on the scores of medical assessment. Kappa coefficient can be interpreted as the ratio is expressed by Equation (5) [14], [15]:
p0 p c 1 pc
(5)
Here, p0 is the proportion of units in which the observers agreed and pc is the proportion of units for which agreement is expected by chance. Kappa’s possible values are ranges from 1 up to 1. The maximum value indicates that the observers agreed for all of examination samples. Landis interpretation on kappa coefficient values can be summarised as shown in Table 1 [15]. TABLE I. AGREEMENT INTERPRETATION OF KAPPA COEFFICIENT Figure 2. Flow diagram of α-PASI erythema assessment
As shown in Figure 2, patients are grouped into dark, brown, light brown or fair skin tones based on the L* values of their normal skin. The classification is performed by using unsupervised clustering algorithm fuzzy c-means (FCM) clustering [12], [13]. Unsupervised clustering algorithm is used since the ground truth of erythema scoring cannot be provided. Scores obtained from dermatologists' assessments has low agreement among the raters. Therefore, its assessment cannot be considered as either reference or ground truth. Two dedicated FCM algorithms are applied consecutively to classify normal skin tone and to score PASI erythema. FCM is a method of clustering which allows a piece of data to belong to two or more clusters. The method is based on minimisation of the following objective function, as given in Equation (2). N
Jm
C
umij xi c j
2
,
1 m
Agreement interpretation