Paris Sud, Paris, France; 3Department of Obstetrics, H ôpital. CHI Creteil ... bleeding, emergent CS (
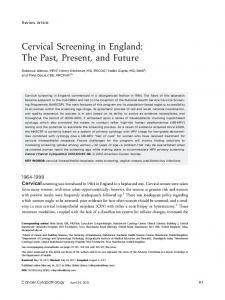
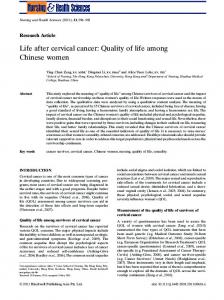
25–28 September 2016, Rome, Italy Methods: Retrospective analysis of early first trimester (6–8 weeks of gestation) ultrasound images of CPS. COS1 insertion was defined as when ≥ two thirds of the A-P diameter of the gestational sac was above the endometrial line, while COS2 when < two thirds of the A-P diameter of the gestational sac was above the endometrial line (see figure). Furthermore, these cases were divided into two different categories according to the presence (COS2+) or not (COS2-) of an intersection between the A-P diameter of the ectopic sac and the endometrial line (see figure). Results: Sixty-eight pregnancies were included in the study. The risk of placenta percreta was significantly higher in pregnancies with COS1 compared to COS2 insertion (OR: 6.67, 95% CI 1.3-33.3; p = 0.001); furthermore, this risk was even higher when comparing cases with COS1 with COS2- (OR: 12.0, 95% CI 1.9-75.7; p = 0.003), while there was no significant risk of developing placenta percreta in women with COS2+ compared to COS2- (OR: 2.28, 95% CI 0.7-7.7; p = 0.2). Women with COS2- had a significant lower risk of developing placenta percreta compared to those with COS1 (OR: 0.069, 95% CI 0.01-0.4). COS1 implantation was independently associated with the occurrence of placenta percreta (OR: 12,849, 95% CI 2.1-13.2). Conclusions: Ultrasound assessment of the relationship between the ectopic gestational sac and the endometrial line may anticipate the natural history of CSP. CSP may not always be associated with adverse outcome and may progress to less severe forms of MAP amenable of post-natal treatment and successful pregnancy outcome.
Supporting information can be found in the online version of this abstract
OP27.02 Assessment of fusion imaging: a new image scoring in the diagnosis of placenta accreta L. Gitz1,2 , C. Touboul3,4 , M. Houllier1,2 , C. Theodore3,4 , M. Gayet5 , M. Senat1,2 , J. Levaillant1,2 Hopital Bicetre, Kremlin Bicˆetre, France; 2 University of ˆ Paris Sud, Paris, France; 3 Department of Obstetrics, Hopital ˆ CHI Creteil, Creteil, France; 4 University of East Paris, Paris, Bicˆetre, Kremlin France; 5 Department of Radiology, Hopital ˆ Bicˆetre, France 1
Objectives: To assess the additional benefit of fusion imaging new scoring in the diagnosis of placenta accreta. Methods: During two years, in two reference centres, patients presenting with a suspicion of placenta accreta were proposed to be screened with ultrasound scan, and MRI, and fusion imaging. We defined a new score features to predict the abnormal placental invasion using fusion imaging. Our score includes 4 categories: intra-placental signs, myometrium signs, vascularisation data and global appearance. Each fusion imaging was analysed prospectively without knowing the results of others exams. The final diagnosis of placenta accreta was obtained by pathological findings or clinical criteria at the time of delivery. Results: Seventeen patients were included with suspect placenta accreta. The final diagnosis of accreta were confirmed after delivery in four cases. The specificity of ultrasound and MRI was 75% and
Short oral presentation abstracts 66% respectively. The positive predictive value was 57% for US and 50% for MRI. The new fusion imaging score showed a specificity of 92% and a positive predictive value of 80%. There was no difference in term of sensibility and negative predictive value which were 80% and 90% respectively for the three exams. New score features using fusion imaging offer a better accuracy of diagnosis in case of placenta accreta suspected by sonography and/or MRI. By combining the advantages of both IRM and US for placenta imaging synchronised on specific suspicious area, added to the possibility of appended Doppler signal on the MRI volume which allowed analyse of placenta vascularisation without any mother injection, fusion imaging improves the diagnosis of placenta accreta. Conclusions: Fusion imaging in the diagnosis of placenta accreta has previously shown good feasibility. Using our new specific score features for fusion imaging will improve the diagnosis of placenta accreta in term of specificity and positive predictive value.
OP27.03 Cervical length as a predictor of placental adherence and massive hemorrhage in placenta previa A.A. Altraigey1 , M.I. Ellaithy2 , A. Majeed2 1 Department
of Obstetrics and Gynecology, Banha University, Qalubeya-Banha, Qalubeya, Egypt; 2 Department of Obstetrics and Gynecology, Ain Shams University, Cairo, Egypt Objectives: To evaluate the relationship between cervical length (CL) and obstetrical outcome in women with placenta previa. Methods: A retrospective chart review was performed for 150 patients who were having medically uncomplicated, singleton pregnancies with an antenatally diagnosed placenta previa. They were categorised based on CL of at/over 30 mm (n = 75) or less (n = 75). Exclusion criteria were threatened preterm labor, multiple gestation, ruptured membranes, evidence of polyhydramnios, fetal growth restriction, fetal anomalies or medical disorders complicating the pregnancy. The outcomes measured were gestational age at delivery, preterm labor before 34 weeks, the use tocolytic agents, antepartum hemorrhage, gestational age at initial bleeding, emergent CS (1000 ml), placental adherence, Caesarean hysterectomy and retained placenta. Perinatal outcomes as birth weight, Apgar score, umbilical pH and neonatal complications were also recorded. Results: Based on the receiver operating characteristic curve, the sensitivity, specificity, positive predictive and negative predictive values were 73.6%, 85.2%, 28.6%, and 96.7%, respectively at a cut-off point 3 cm CL for predicting cases at high risk for placental adherence. The sensitivity, specificity, positive predictive and negative predictive values were 52.2, 86.0, 14.0, and 89.7%, respectively, for the prediction of massive hemorrhage. The estimated blood loss at CS and the rate of Caesarean hysterectomy were significantly higher in the shorter CL group in our study. Conclusions: As its strong relationship to emergent CS, Caesarean hysterectomy, intraoperative estimated blood loss and placental adherence, cervical length measurements should be a fundamental step in the assessment of a pregnancies complicated with placenta previa.
© The Authors 2016 © Ultrasound in Obstetrics & Gynecology 2016; 48 (Suppl. 1): 51–166.
139