17th IFAC Symposium on System Identification 17th IFAC Symposium on Identification 17th IFAC Symposium on System SystemCenter Identification Beijing International Convention Available online at www.sciencedirect.com Beijing International Convention 17th IFAC Symposium on SystemCenter Identification Beijing International Convention Center October 19-21, 2015. Beijing, China OctoberInternational 19-21, 2015. 2015. Convention Beijing, China China Beijing Center October 19-21, Beijing, October 19-21, 2015. Beijing, China
ScienceDirect
IFAC-PapersOnLine 48-28 (2015) 1381–1385
Assessing Assessing Standing Standing Balance Balance using using MIMO MIMO Assessing Standing Balance using MIMO Closed Closed Loop Loop System System Identification Identification Techniques Techniques Closed Loop System Identification Techniques
Jantsje Jantsje H. H. Pasma*. Pasma*. Denise Denise Engelhart**. Engelhart**. Andrea Andrea B. B. Maier***. Maier***. Carel Carel G.M. G.M. Meskers Meskers ****. ****. Ronald G.K.M. Aarts *****. Alfred C. Schouten ******. Herman van der Kooij *******. Jantsje G.K.M. H. Pasma*. Denise Engelhart**. Andrea B. Maier***. Carel Meskers ****. Ronald Aarts *****. Alfred ******. Herman van der *******. Ronald G.K.M. Aarts *****. Alfred C. C. Schouten Schouten ******. Herman vanG.M. der Kooij Kooij *******. Ronald G.K.M. Aarts *****. Alfred C. Schouten ******. Herman van der Kooij *******.
*Department *Department of Rehabilitation Medicine, Leiden University Medical Center, Leiden, the Netherlands, Department of *Department of of Rehabilitation Rehabilitation Medicine, Medicine, Leiden Leiden University University Medical Medical Center, Center, Leiden, Leiden, the the Netherlands, Netherlands, Department Department of of Engineering, Delft University of Technology, Delft, the Netherlands, *Department of Biomechanical Rehabilitation Medicine, Leiden University Medical Center, Leiden, the Netherlands, Department of Biomechanical Engineering, Delft University of Technology, Delft, the Netherlands, Biomechanical Engineering, Delft University of Technology, Delft, the Netherlands, (Tel:+31 70 526 3710, e-mail:
[email protected],
[email protected]) Biomechanical Engineering, Delft University of Technology, Delft, the Netherlands, (Tel:+31 70 526 3710, e-mail:
[email protected],
[email protected]) (Tel:+31 70 526 3710, e-mail:
[email protected],
[email protected]) **Department of Biomechanical Engineering, MIRA Institute for Biomedical Technology and Technical Medicine, University (Tel:+31 70 526 3710, e-mail:
[email protected],
[email protected]) **Department Engineering, MIRA Institute for and **Department of of Biomechanical Biomechanical Engineering, MIRA Institute for Biomedical Biomedical Technology Technology and Technical Technical Medicine, Medicine, University University of Twente, Enschede, the Netherlands, (e-mail:
[email protected]) **Department of Biomechanical Engineering, Institute for (e-mail: Biomedical Technology and Technical Medicine, University of Enschede, the
[email protected]) of Twente, Twente, Enschede,MIRA the Netherlands, Netherlands, (e-mail:
[email protected]) *** section Geriatrics and VU Twente, Enschede, Netherlands, (e-mail:
[email protected]) *** Department of Internal Medicine, section of Geriatrics and Gerontology, VU University Medical Center, Amsterdam, the *** Department Department of of Internal InternalofMedicine, Medicine, section of ofthe Geriatrics and Gerontology, Gerontology, VU University University Medical Medical Center, Center, Amsterdam, Amsterdam, the the Netherlands,(e-mail:
[email protected]) *** Department of Internal Medicine, section of Geriatrics and
[email protected]) Gerontology, VU University Medical Center, Amsterdam, the Netherlands,(e-mail:
[email protected]) Netherlands,(e-mail: **** Medicine, Medical Netherlands,(e-mail:
[email protected]) **** Department Department of of Rehabilitation Rehabilitation Medicine, VU VU University University Medical Center, Center, Amsterdam, Amsterdam, the the Netherlands, Netherlands, **** Department of Rehabilitation Medicine, VU University Medical Center, Amsterdam, the Netherlands, (e-mail:
[email protected]) **** Department of Rehabilitation Medicine, VU University Medical Center, Amsterdam, the Netherlands, (e-mail:
[email protected]) (e-mail:
[email protected]) ***** Department of Mechanical(e-mail: Automation, University of Twente, Enschede, the Netherlands,
[email protected]) ***** University ***** Department Department of of Mechanical Mechanical Automation, Automation, University of of Twente, Twente, Enschede, Enschede, the the Netherlands, Netherlands, (e-mail:
[email protected]) ***** Department of Mechanical Automation, University of Twente, Enschede, the Netherlands, (e-mail:
[email protected]) (e-mail:
[email protected]) ****** Department of Biomechanical Engineering, Delft University of Technology, Delft, the Netherlands, (e-mail:
[email protected]) ****** Engineering, Delft ****** Department Department of of Biomechanical Biomechanical Engineering, Delft University University of of Technology, Technology, Delft, Delft, the the Netherlands, Netherlands, (e-mail:
[email protected]) ****** Department of Biomechanical(e-mail: Engineering, Delft University of Technology, Delft, the Netherlands,
[email protected]) (e-mail:
[email protected]) ******* MIRA (e-mail:
[email protected]) ******* Department of Biomechanical Engineering, MIRA Institute for Biomedical Technology and Technical Medicine, ******* Department Department of of Biomechanical Biomechanical Engineering, Engineering, MIRA Institute Institute for for Biomedical Biomedical Technology Technology and and Technical Technical Medicine, Medicine, University of Twente, Enschede, the Netherlands,(e-mail:
[email protected]) ******* Department of Biomechanical Institute for Biomedical Technology and Technical Medicine, University of Twente, Twente, Engineering, Enschede, the theMIRA Netherlands,(e-mail:
[email protected]) University of Enschede, Netherlands,(e-mail:
[email protected]) University of Twente, Enschede, the Netherlands,(e-mail:
[email protected]) Abstract: Abstract: Human Human standing standing balance balance is is aaa complex complex of of systems, systems, like like the the muscles, muscles, nervous nervous system system and and Abstract: Human standing balance is complex of systems, like the muscles, nervous system and sensory systems, interacting with each other in a closed loop to maintain upright stance. With Abstract: Humaninteracting standing balance is aother complex systems, the muscles, nervous and sensory systems, systems, interacting with each each other in aa of closed loop like to maintain maintain upright stance.system With age, age, sensory with in closed loop to upright stance. With age, disease and medication use these deteriorate, which could result in upright impairedstance. balance. In this sensory systems, interacting with systems each other in a closed loop to maintain With disease medication use systems deteriorate, which could result In this disease and and medication use these these systems deteriorate, which could result in in impaired impaired balance. balance. In age, this paper, it is demonstrated that multi-input-multi-output closed loop system identification techniques disease and medication use these systems deteriorate, which could result in impaired balance. In this paper, it is demonstrated that multi-input-multi-output closed loop system identification techniques paper, it is demonstrated that multi-input-multi-output closed loop system identification techniques (MIMO-CLSIT) can be used to assess the underlying systems involved in standing balance and guide paper, it is demonstrated that multi-input-multi-output closed loop system identification techniques (MIMO-CLSIT) can be used to assess the underlying systems involved in standing balance and guide (MIMO-CLSIT) can be used to assess the underlying systems involved in standing balance and guide possible therapeutic this study, mechanical and sensory perturbations combined and (MIMO-CLSIT) can options. be used In to assess the underlying involved in standingwere balance and guide possible therapeutic options. In this mechanical and perturbations were combined and possible therapeutic options. In this study, study, mechanicalsystems and sensory sensory perturbations were combined and applied simultaneously using a Balance test Room. The results demonstrate the value of MIMO-CLSIT possible therapeutic options. In this study, mechanical and sensory perturbations were combined and applied simultaneously using a Balance test Room. The results demonstrate the value of MIMO-CLSIT applied simultaneously using a Balance test Room. The results demonstrate the value of MIMO-CLSIT to assess the underlying systems involved in standing balance and therefore to improve diagnosis of applied simultaneously using a Balance test Room. The results demonstrate the value of MIMO-CLSIT to assess the underlying systems involved in standing balance and therefore to improve diagnosis to assess the underlying systems involved in standing balance and therefore to improve diagnosis of of impaired standing balance. to assess standing the underlying impaired standing balance.systems involved in standing balance and therefore to improve diagnosis of impaired balance. impaired standing balance. Federation of © 2015, IFAC (International Automatic Control) Hosting by Elsevier Ltd. All rights reserved. Keywords: Keywords: Closed-loops, Closed-loops, Perturbation, Perturbation, MIMO, MIMO, System System identification, identification, Diagnosis Diagnosis Keywords: Closed-loops, Perturbation, MIMO, System identification, Diagnosis Keywords: Closed-loops, Perturbation, MIMO, System identification, Diagnosis each joint to keep the body in an upright position (Engelhart each each joint joint to to keep keep the the body body in in an an upright upright position position (Engelhart (Engelhart 1. 1. INTRODUCTION INTRODUCTION 1. INTRODUCTION et al. 2014a). The human balance control could compared each joint to keep the body in an upright et al. 2014a). The human balance control could be compared et al. 2014a). The human balance control position could be be (Engelhart compared 1. INTRODUCTION to robot stance control, in which typically zero moment point et al. 2014a). human control could be compared to robot stanceThe control, in balance which typically typically zero moment moment point Impaired standing balance is a significant problem in elderly Impaired standing balance is a significant problem in elderly to robot stance control, in which zero point Impaired standing balance is a significant problem in elderly compensation is used. However, flexible sensory integration and is one of the main causes and risk factors of falling (Lin to robot stanceis in which typically zero moment point compensation iscontrol, used. However, However, flexible sensory sensory integration Impaired standing balance is a significant problem in elderly and is one of the main causes and risk factors of falling (Lin compensation used. flexible integration and is one of the main causes and risk factors of falling (Lin is not included, resulting in instability of a robot in situations et al. 2012; Muir et al. 2010; Rubenstein 2006). These falls compensation used. However, flexible is not not included, included,isresulting resulting in instability instability of aasensory robot in inintegration situations and is one of the main causes and risk factors of falling (Lin et al. 2012; Muir et al. 2010; Rubenstein 2006). These falls is in of robot situations et al. 2012; Muir et al. 2010; Rubenstein 2006). These falls in which a human is able to maintain standing balance could result in serious injuries and finally in death included, resulting in instability of a robot in situations in which aa human is to standing balance et al. 2012; al. 2010; Rubenstein falls is could result in injuries and finally in in not which human is able able to maintain maintain standing balance could resultMuir in etserious serious injuries and 2006). finally These in death death (Peterka 2009). in which a human is able to maintain standing balance (Peterka 2009). (Cummings et al. 1985). In combination with the increasing could result in serious injuries and finally in death (Cummings et al. 1985). In combination with the increasing (Peterka 2009). (Cummings et al. 1985). In combination with the increasing (Peterka 2009). population of elderly and the increased average life (Cummings 1985). In with the increasing population et of al.elderly elderly andcombination the increased increased average life With age, disease and medication use, the underlying systems population of and the average life With age, age, disease disease and and medication medication use, use, the the underlying underlying systems systems expectancy, falls and are huge population and thebalance increased life With expectancy, of fallselderly and impaired impaired balance are aaa average huge sociosociodeteriorate (Horak et al. 1989; Konrad et al. 1999; Sturnieks expectancy, falls and impaired balance are huge socioWith age, disease and medication use, the underlying systems deteriorate (Horak et al. 1989; Konrad et al. 1999; Sturnieks deteriorate (Horak et al. 1989; Konrad et al. 1999; Sturnieks economic problem (Hartholt et al. 2012). expectancy, falls and impaired balance are a huge socioeconomic problem problem (Hartholt (Hartholt et et al. al. 2012). 2012). economic et al. 2008). As the underlying systems interact with deteriorate (Horak et al. 1989; Konrad et al. 1999; Sturnieks et al. 2008). As the underlying systems interact with each et al. 2008). As the underlying systems interact with each each economic problem (Hartholt et al. 2012). other in a closed loop, they can compensate for each other’s et al. 2008). As the underlying systems interact with each other in a closed loop, they can compensate for each other’s Standing balance is the ability to maintain an upright position Standing balance is the ability to maintain an upright position other in a closed loop, they can compensate for each other’s Standing balance is the ability to maintain an upright position deterioration. This makes difficult to underlying and to counteract disturbances, such as gravity. To keep the other in a closed loop, they it compensate for each other’s deterioration. This makes itcan difficult to detect detect underlying Standing balance is the ability to maintain an upright position and to counteract disturbances, such as gravity. To keep the deterioration. This makes it difficult to detect underlying and to counteract disturbances, such as gravity. To keep the changes in standing balance and underlying causes of body upright, several systems interact in a closed loop to deterioration. This makes it difficult to detect underlying changes in in standing standing balance and underlying underlying causes of of and counteract disturbances, as gravity. To keep body several systems interact in loop to balance and causes bodytoupright, upright, several systems such interact in aa closed closed loop the to changes impaired standing balance using current descriptive clinical changes in standing balance and underlying causes of impaired standing balance using current descriptive clinical control each joint, like the ankles and hips, resulting in a body upright, several systems interact in a closed loop to control each joint, like the ankles and hips, resulting in a impaired standing balance using current descriptive clinical control each joint, like the ankles and hips, resulting in a balance tests (Pasma et al. 2014). Therefore, a new method is impaired standing balance using current descriptive clinical balance tests (Pasma et al. 2014). Therefore, a new method multi-segmental system. The central nervous system receives control each joint, like The the ankles hips,system resulting in a balance tests (Pasma et al. 2014). Therefore, a new method is multi-segmental system. central nervous receives is multi-segmental system. The central and nervous system receives required to detect the in standing balance balance tests (Pasma etunderlying al. 2014).changes Therefore, a new method is required to detect the underlying changes in standing balance information about the velocity and position of all body multi-segmental system. The central nervous system receives information about the velocity and position of all body required to detect the underlying changes in standing balance information about the velocity and position of all body at an early stage resulting in a specific diagnosis of impaired required to detect the underlying changes in standing balance at an early stage resulting in a specific diagnosis of impaired segments from the sensory systems, such as the visual, informationfrom about velocity and position body at an early stage resulting in a specific diagnosis of impaired segments from the the sensory systems, such as asofthe theallvisual, visual, segments the sensory systems, such standing balance and aaa possibility to targeted an early stage resulting in a specific diagnosis of impaired standing balance and therefore possibility to apply targeted vestibular and proprioceptive system, and segments from sensory systems, the visual, at vestibular and the proprioceptive system,such andasforce-related force-related standing balance and therefore therefore possibility to apply apply targeted vestibular and proprioceptive system, and force-related interventions to improve standing balance. and Golgi-tendon standing balance and therefore a possibility to apply targeted interventions to improve standing balance. sensory information from tactile sensors vestibular and proprioceptive system, and force-related sensory information from tactile sensors Golgi-tendon sensory information from tactile sensors and Golgi-tendon interventions to improve standing balance. organs. In the CNS, this information is integrated based on interventions to improve standing balance. sensory information from tactile sensors and Golgi-tendon organs. In the CNS, this information is integrated based on organs. In the CNS, this information is integrated based on Previous Previous research research already already showed showed that that it it is is possible possible to to the reliability aa motor command is to the based muscles. research already showed that it is possible to organs. In the and CNS, this information is sent integrated on Previous the and command sent to the reliability reliability and a motor motor command is is sent to the the muscles. muscles. describe underlying mechanisms involved in standing Previous showed involved that it is in to describe research underlyingalready mechanisms involved inpossible standing The muscles contract and generate a corrective torque around describe underlying mechanisms standing the and a motor command is sent totorque the muscles. The muscles and aa corrective around Thereliability muscles contract contract and generate generate corrective torque around describe underlying mechanisms involved in standing The muscles contract and generate a corrective torque around 2405-8963 © 2015, IFAC (International Federation of Automatic Control) Hosting by Elsevier Ltd. All rights reserved.
Copyright IFAC 2015 1381 Peer review© of International Federation of Automatic Copyright © IFAC 2015 1381 Copyright ©under IFAC responsibility 2015 1381Control. 10.1016/j.ifacol.2015.12.325 Copyright © IFAC 2015 1381
2015 IFAC SYSID 1382 October 19-21, 2015. Beijing, China
Jantsje H. Pasma et al. / IFAC-PapersOnLine 48-28 (2015) 1381–1385
balance using perturbations and multi-input-multi-output closed loop system identification techniques (MIMO-CLSIT) (Boonstra et al. 2013; Engelhart et al. 2014b; Peterka 2002). In those studies, several systems were perturbed one by one during quiet stance, while the subject kept his balance. The reaction of the human body was measured by the joint angles and torques and related to the perturbation using nonparametric system identification methods, which shows to be the most robust way to estimate balance behaviour (Engelhart et al. 2015). In this paper, we show it is possible to apply multiple mechanical and sensory perturbation signals simultaneously to the human body and therefore to detect underlying systems involved in standing balance in one test using MIMO-CLSIT. The design of a custom-made device, the Balance Test Room (BalRoom), is introduced, which is used to apply the several perturbations simultaneously during standing balance.
hip joint and their coupling in standing balance (Engelhart et al. 2014b). The BalRoom was controlled using xPC target and a custommade Matlab interface. 2.2 Perturbation signals To distinguish the reaction of the human body on each perturbation and therefore the contribution of each underlying system involved in standing balance, independent multisines were designed with a unique combination of frequencies (Figure 2). All excited frequencies were multiples of 0.0625 Hz resulting in a period of 16 s. Both support surfaces rotated following a continuous position perturbation signal with increasing zero-to-peak amplitude over trials and a flat velocity spectrum with frequencies between 0.125 and 6.9375 Hz. The visual scene rotated following a continuous position perturbation signal with constant zero-to-peak amplitude of 0.03 radians and a flat velocity spectrum with frequencies between 0.0625 and 1 Hz. Both rods moved following an independent, continuous force perturbation signal represented by zippered multisines with constant zero-to-peak amplitude of 30 Newton and consist of independent frequency contents between 0.75 and 7 Hz. 2.3 Participants
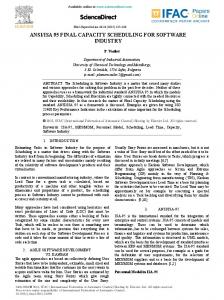
Figure 1: The Balance Test Room (BalRoom) set up consisting of support surfaces and a visual scene to apply sensory perturbations and rods on hip and shoulder level to apply mechanical perturbations to the human body.
The BalRoom was evaluated on 5 healthy participants (age 25.8 ± 2.8, 3 women). All participants gave written informed consent before entry to the study. 2.4 Procedure The BalRoom was used to simultaneously perturb the visual information by VS rotation, the proprioceptive information by SS rotation around the ankle axes and the leg and trunk segment by giving pushes and pulls using a rod at the hip and shoulder level.
2. METHODS 2.1 Apparatus The BalRoom is a custom-made device (MotekforceLink, the Netherlands and University of Twente, the Netherlands) to study standing balance. The BalRoom consists of three modules applying perturbations simultaneously during standing balance (Figure 1). The first module consists of two support surfaces (SS), which rotate around the ankle axes. Both support surfaces are actuated independently. By these rotations a sensory perturbation to the proprioceptive system is applied (Schouten et al. 2011). The second module consists of a visual scene (VS), which rotates around the ankle axes and perturbs the visual information. Both perturbations allow to assess the contribution of the sensory systems in standing balance (Peterka 2002). The third module consists of two rods applying pushes and pulls at the hip and between the shoulder blades. By these perturbations the leg and trunk segment will move, which makes it possible to assess the contribution of the ankle and
During all experiments the participant wore comfortable flat shoes. The participant was instructed to stand with the arms resting along the side with both feet on the support surfaces. Three trials were presented in random order with increasing perturbation amplitude of the SS rotation (i.e. 0.02, 0.03 and 0.04 radians), while the amplitude of the other perturbations remained constant. The perturbation signals were repeated 8 times resulting in trials of 128 seconds (i.e. 8 times 16 seconds). Before starting the recording of each trial the participant was given about 10 seconds to get accustomed to the perturbations. Between trials, the participant was offered ample resting time depending on individual needs. The participant wore a safety harness to prevent falling, which did not constrain movement and did not provide support or orientation information.
1382
2015 IFAC SYSID October 19-21, 2015. Beijing, China
Jantsje H. Pasma et al. / IFAC-PapersOnLine 48-28 (2015) 1381–1385
d
1383
S x ( f ) = Φ d , x ( f ) ⋅ [Φ d , d ( f )]
−1
(1)
In which Φd,x represents the CSD of the perturbation (d) (i.e. support surface (SS) rotation or visual scene (VS) rotation) and x, which represents the ankle torque (Ta), hip torque (Th), leg angle (θl), or hip angle (θh), and Φd,d the PSD of the perturbation. This results in 8 FRFs; SS rotation to 1) ankle torque (SSSTa), 2) hip torque (SSSTh), 3) leg angle (SSSθl), and 4) hip angle (SSSθh), and 5) t/m 8) the VS rotation to each torque and angle (VSSTa,VSSTh VSSθl,VSSθh). Each FRF is represented by a magnitude and phase representing the relation between perturbation and torque or angle in terms of amplitude and time. Joint dynamics The MIMO approach was used to estimate the dynamics of the ankle and hip joint and their coupling according to (2) (Engelhart et al. 2014b). Figure 2: Normalized time signals of the perturbations of the support surfaces (SS), the visual scene (VS) and the rods applying forces at hip and shoulder level. 2.5 Data recording and processing The actual angles of SS rotation (i.e. motor angles), the applied torques to both support surfaces (i.e. motor torques) and the applied forces to the hip and shoulder (i.e. push forces) were available for measurement. Lower and upper body segmental movements were measured in anteriorposterior direction using two draw wire potentiometers (Celesco SP2-50, Celesco, Chatsworth, CA, United States) at a sample frequency of 1000 Hz. The leg and hip angle were calculated using goniometric and using the segment movement of the lower and upper body. The ankle and hip torque were obtained from the motor torques and push forces using inverse dynamics (Winter et al. 1990). The time series were segmented into eight data blocks of 16 seconds (i.e. the period of the perturbation signal). 2.6 Closed loop system identification techniques MIMO-CLSIT was used to estimate the contribution of the sensory systems and the dynamics of the ankle and hip joint. To indicate the effect of the perturbations on the ankle torque, hip torque, leg angle and hip angle, Frequency Response Functions (FRFs) were estimated using non-parametric methods. The time series of the perturbations, ankle and hip torque, and leg and hip angle were transformed to the frequency domain. The periodic part of the frequency coefficients was determined by averaging over the data blocks. The Power Spectral Densities (PSD) and Cross Spectral Densities (CSD) were computed to calculate the FRFs (van der Kooij et al. 2005). Only the excited frequencies were analysed. Sensitivity functions The sensitivity functions were estimated using the indirect approach according to (1) (Peterka 2002; van der Kooij et al. 2005).
H c = − S d ,T (S d ,θ )
−1
(2)
In which Sd,T and Sd,θ are the CSD matrices between the external perturbations (d) and the corrective ankle and hip torques (T) and the leg and hip angles (θ) resulting in a twoby-two matrix (Hc). This matrix represents 4 FRFs; 1) leg angle to ankle torque (Hθl2Ta), 2) hip angle to ankle torque (Hθh2Ta), 3) hip angle to hip torque (Hθh2Th), and 4) leg angle to hip torque (Hθl2Th). Each FRF is represented by a magnitude and phase representing the relation in terms of amplitude and time. 3. RESULTS In this section we demonstrate the application of the BalRoom by identifying the contribution of the sensory systems and the joint dynamics. Figure 3 shows the sensitivity functions of the SS rotations to ankle and hip torques and angles averaged over 5 healthy participants by increasing the perturbation amplitude of the SS rotation. The magnitude of the sensitivity functions decreases with increasing perturbation amplitude, indicating that participants react less on the proprioceptive perturbation by using their proprioceptive information less (downweighting). Figure 4 shows the averaged sensitivity functions of the VS rotation to ankle and hip torques and angles by increasing the perturbation amplitude of the SS rotation. In this case the magnitude increased with increasing perturbation amplitude, indicating that participants react more on the visual information by using their visual information more (upweighting). Figure 5 shows the averaged joint dynamics (Hθl2Ta and Hθh2Th) and their coupling (Hθl2Th and Hθh2Ta) during simultaneous perturbation of the visual and proprioceptive information and the leg and trunk segment of 5 healthy participants. It is shown that the joint dynamics and their coupling remained constant by changing the perturbation amplitude of the sensory perturbations.
1383
2015 IFAC SYSID 1384 October 19-21, 2015. Beijing, China
Jantsje H. Pasma et al. / IFAC-PapersOnLine 48-28 (2015) 1381–1385
4.1 Application Combining SS rotation with VS rotation makes it possible to assess the contribution of the proprioceptive and visual system in maintaining standing balance at the same time. According to the sensory reweighting hypothesis, a flexible and adaptive process of combining the sensory information based on their reliability, the results showed a decrease in sensitivity to the SS rotation by increasing the amplitude of the SS rotation accompanied with an increase in sensitivity to the VS rotation. This indicates that the proprioceptive information is weighted less accompanied with more weighting of the visual information in case of proprioceptive perturbations (Peterka 2002).
Figure 3: Averaged Frequency Response Functions of the sensitivity functions of support surface (SS) rotations to the ankle torque, hip torque, leg angle and hip angle for three conditions with increasing perturbation amplitude of the SS rotation. 4. DISCUSSION In this study we investigated the value of MIMO-CLSIT to assess the underlying systems involved in standing balance using a novel apparatus, which can perturb the proprioceptive information, visual information, and ankle and hip segment simultaneously. Independent sensory and force perturbations were applied simultaneously, while the participant maintained standing balance. The results showed that using MIMO-CLSIT the underlying systems in standing balance can be investigated in one test. By applying multiple sensory and mechanical perturbations simultaneously, both the contribution of the sensory systems and the joint dynamics and their coupling can be assessed at the same time. The results are according to previous studies in which the same kind of perturbations were applied one by one (Engelhart et al. 2014b; Peterka 2002). However, this is the first study in which these perturbations were applied simultaneously. Compared with Peterka (2002) increasing the perturbation amplitude of the SS rotation results in a decrease of the magnitude of the sensitivity functions of the SS rotation and an increase of the magnitude of the sensitivity functions of the VS rotation. Results of the joint dynamics and their coupling were comparable with Engelhart et al. (2014b). These results indicate that unless applying mechanical and sensory perturbations simultaneously, it is still possible to detect the contribution of the sensory systems and the joint dynamics and their coupling. The next step is to describe the control of standing balance by a multi-segmental model consisting of the underlying systems and an ankle and hip joint, which will give physiological meaning to the measured frequency response functions using estimated model parameters. Previous studies already indicated that it is possible to describe the underlying systems by estimated parameters using balance control models in case of a single perturbation (Peterka 2002).
The application of the perturbation of the leg and trunk segment makes it possible to investigate the dynamics of the hip and ankle joint and their coupling (Boonstra et al. 2013; Engelhart et al. 2014b). 4.2 Clinical implications The results of this study show the value of use MIMO-CLSIT to assess the underlying systems involved in standing balance. This shows that using this technique it is possible to disentangle the underlying systems, which is not possible using current clinical balance tests. Therefore, this study shows the value of this technique in detecting the underlying cause of impaired standing balance in clinical practice. A more specific and differential diagnosis of impaired standing balance makes it possible to develop and implement targeted interventions to improve standing balance and finally reduce falling. Furthermore, the BalRoom and MIMO-CLSIT are applicable to investigate the effect of new developed interventions. The contribution of the underlying systems can be measured before and after interventions and will show the changes in the underlying systems involved in standing balance due to the intervention. Besides, this technique can be used to monitor treatment effects.
Figure 4: Averaged Frequency Response Functions of the sensitivity functions of visual scene (VS) rotation to the ankle torque, hip torque, leg angle and hip angle for three conditions with increasing amplitude of the support surface rotation.
1384
2015 IFAC SYSID October 19-21, 2015. Beijing, China
Jantsje H. Pasma et al. / IFAC-PapersOnLine 48-28 (2015) 1381–1385
4.3 Conclusions
1385
identification technique. IEEE Trans.Neural Syst.Rehabil.Eng
In this study, mechanical and sensory perturbations were applied simultaneously to assess standing balance in one test using a novel apparatus, which can perturb the proprioceptive information, visual information, and ankle and hip segment simultaneously. The results show the possibility to apply MIMO-CLSIT to disentangle underlying systems in human standing balance, in which current clinical balance tests are lacking. Therefore, MIMO-CLSIT is an essential tool to improve diagnosis of impaired standing balance in clinical practice and to implement targeted interventions to improve standing balance. The next step is to describe the underlying systems involved in standing balance by estimating model parameters using a multi-segmental balance control model.
Hartholt, K.A., Polinder, S., Van der Cammen, T.J., Panneman, M.J., Van, d., V, Van Lieshout, E.M., Patka, P., and Van Beeck, E.F. 2012. Costs of falls in an ageing population: a nationwide study from the Netherlands (20072009). Injury, 43, (7) 1199-1203 Horak, F.B., Shupert, C.L., and Mirka, A. 1989. Components of postural dyscontrol in the elderly: a review. Neurobiol.Aging., 10, (6) 727-738 Konrad, H.R., Girardi, M., and Helfert, R. 1999. Balance and aging. Laryngoscope, 109, (9) 1454-1460 Lin, H.W. and Bhattacharyya, N. 2012. Balance disorders in the elderly: epidemiology and functional impact. Laryngoscope., 122, (8) 1858-1861 Muir, S.W., Berg, K., Chesworth, B., Klar, N., and Speechley, M. 2010. Quantifying the magnitude of risk for balance impairment on falls in community-dwelling older adults: a systematic review and meta-analysis. J.Clin.Epidemiol., 63, (4) 389-406
Figure 5: Averaged Frequency Response Functions of the dynamics of the ankle and hip joint (Hθl2Ta and Hθh2Th) and their coupling (Hθl2Th and Hθh2Ta).
Pasma, J.H., Engelhart, D., Schouten, A.C., van der Kooij, H., Maier, A.B., and Meskers, C.G. 2014. Impaired standing balance: the clinical need for closing the loop. Neuroscience, 267, 157-165 Peterka, R.J. 2002. Sensorimotor integration in human postural control. J Neurophysiol., 88, (3) 1097-1118
REFERENCES Boonstra, T.A., Schouten, A.C., and van der Kooij, H. 2013. Identification of the contribution of the ankle and hip joints to multi-segmental balance control. J.Neuroeng.Rehabil., 10, 23
Peterka, R.J. 2009. Comparison of human and humanoid robot control of upright stance. J.Physiol Paris, 103, (3-5) 149-158 Rubenstein, L.Z. 2006. Falls in older people: epidemiology, risk factors and strategies for prevention. Age Ageing., 35 Suppl 2:ii37-ii41., ii37-ii41
Cummings, S.R., Kelsey, J.L., Nevitt, M.C., and O'Dowd, K.J. 1985. Epidemiology of osteoporosis and osteoporotic fractures. Epidemiol.Rev., 7, 178-208 Engelhart, D., Boonstra, T. A., Aarts, R. G., Schouten, A. C., and van der Kooij, H. Comparison of closed loop system identification techniques to quantify multi-joint human balance control. 2015. Ref Type: Unpublished Work Engelhart, D., Pasma, J.H., Schouten, A.C., Meskers, C.G., Maier, A.B., Mergner, T., and van der Kooij, H. 2014a. Impaired standing balance in elderly: a new engineering method helps to unravel causes and effects. J Am Med Dir.Assoc., 15, (3) 227-6
Schouten, A.C., Boonstra, T.A., Nieuwenhuis, F., Campfens, S.F., and van der Kooij, H. 2011. A bilateral ankle manipulator to investigate human balance control. IEEE Trans.Neural Syst Rehabil.Eng., 19, (6) 660-669 Sturnieks, D.L., St, G.R., and Lord, S.R. 2008. Balance disorders in the elderly. Neurophysiol.Clin., 38, (6) 467-478 van der Kooij, H., van, A.E., and van der Helm, F.C. 2005. Comparison of different methods to identify and quantify balance control. J Neurosci Methods., 145, (1-2) 175-203 Winter, D.A., Patla, A.E., and Frank, J.S. 1990. Assessment of balance control in humans. Med Prog.Technol., 16, (1-2) 31-51
Engelhart, D., Schouten, A.C., Aarts, R.G., and van der Kooij, H. 2014b. Assessment of multi-joint coordination and adaptation in standing balance: a novel device and system 1385