Social and Behavioral
The Influence of Parenting Change on Pediatric Weight Control Richard I. Stein,* Leonard H. Epstein, Hollie A. Raynor,† Colleen K. Kilanowski, and Rocco A. Paluch
Abstract STEIN, RICHARD I., LEONARD H. EPSTEIN, HOLLIE A. RAYNOR, COLLEEN K. KILANOWSKI, AND ROCCO A. PALUCH. The influence of parenting change on pediatric weight control. Obes Res. 2005;13:1749 –1755. Objective: Parenting style was examined as a predictor of weight loss maintenance in behavioral family-based pediatric obesity treatment. Research Methods and Procedures: Fifty obese children who participated in a behavioral family-based pediatric obesity treatment were studied. Hierarchical regression tested the incremental effect of baseline parenting and parenting during treatment on children’s percentage overweight change over 12 months, beyond demographics and adherence to targeted behaviors. Results: Children’s percentage overweight significantly decreased at 6 (⫺16.3) and 12 (⫺11.1) months. Adherence to program goals significantly increased variance accounted for in the regression model by 10.8%, whereas adding baseline father acceptance and change in father acceptance accounted for another 20.5%. The overall model accounted for 40.6% of the variance in pediatric weight control. ANOVA showed significantly greater percentage overweight decrease from baseline for youth with fathers who increased their acceptance vs. those who decreased acceptance at 6 (⫺19.8 vs. ⫺14.6) and 12 (⫺17.4 vs. ⫺8.1) months. Discussion: Youth who perceive an increase in father ac-
Received for review May 11, 2004. Accepted in final form July 28, 2005. The costs of publication of this article were defrayed, in part, by the payment of page charges. This article must, therefore, be hereby marked “advertisement” in accordance with 18 U.S.C. Section 1734 solely to indicate this fact. Department of Pediatrics, School of Medicine and Biomedical Sciences, State University of New York at Buffalo, Buffalo, New York. *Present address: Center for Human Nutrition, Washington University School of Medicine, St. Louis, Missouri. †Present address: Weight Control and Diabetes Research Center, Brown University/The Miriam Hospital, Providence, Rhode Island. Address correspondence to Leonard H. Epstein, Department of Pediatrics, School of Medicine and Biomedical Sciences, State University of New York at Buffalo, Farber Hall, Room G56, 3435 Main Street, Building 26, Buffalo, NY 14214-3000. E-mail:
[email protected] Copyright © 2005 NAASO
ceptance after treatment had better changes in percentage overweight over 12 months than youth with lower ratings of father acceptance. Future directions include examining how other parenting dimensions impact pediatric obesity treatment outcome and how parental acceptance can be enhanced to improve child weight control. Key words: child, parenting, weight loss
Introduction Parental training is one important component of familybased behavioral treatment programs for pediatric obesity (1). As the child’s primary caregivers and disciplinarians, parents are in a unique position to support their children’s efforts. Parents can control the family’s home environment to promote the child’s healthy behaviors (e.g., eating nutrient-dense foods, avoiding high-calorie foods, and engaging in increased physical activity), and parents can use behavioral strategies to encourage the child’s efforts at behavioral change. Parenting behaviors are one of the main components of behavioral family-based pediatric obesity treatment programs (2), along with nutrition, physical activity, and other weight-control behaviors such as self-monitoring (1). The parenting component of these programs typically includes education in general child management strategies (3), strategies for helping the child meet program demands (4), and specific behavioral techniques such as behavioral contingencies, modeling, environmental control, and reinforcement (5) that both parents can do to encourage healthy weight loss behaviors. The influence of parents on pediatric weight control has been studied in numerous ways. Having the parent serve as an active participant in child weight control, including targeting the parent for behavior change and weight control, is associated with long-term maintenance of pediatric weight control (6). Providing initial training in behavioral parenting methods improved weight control over 1 year in comparison with pediatric weight control without additional parent training (3). Training parents to use positive reinforcement to motivate their children to make behavior change was OBESITY RESEARCH Vol. 13 No. 10 October 2005
1749
Parenting Style and Child Weight Loss, Stein et al.
associated with superior weight loss in comparison with using negative reinforcement methods (7). Families assigned to a mastery-based behavioral intervention, which included mastery of weight control and related behaviors and parent mastery of parenting skills, improved weight control over 1 year compared with a treatment that taught the same material but without mastery (2). Golan et al. (8) showed better weight control if the parent was provided training in parenting and environmental control than if the child was targeted for weight loss, indicating the powerful influence of changes in parent behavior on child’s weightrelated behaviors. Investigators have examined parental individual differences that impact outcome of behavioral pediatric obesity programs and have shown that parent psychopathology (9) and a disorganized/chaotic family environment (10) predict more negative outcome. Parenting style has been examined as a predictor of other youth health behavior and psychological outcomes. Two parenting styles, parental acceptance and a firm parenting style, have been consistently related to outcomes such as increased regimen compliance and glycemic control among children with type I diabetes (11), reduced substance abuse among adolescents (12), and psychological well-being and reduced behavioral problems (13). Parental acceptance and a firm parenting style have been defined as an authoritative parenting style. The parenting strategies highlighted in many behavioral family-based weight loss programs emphasize changes in acceptance of behavior and a firm parenting style, such as both parents taking control over the home environment, monitoring the child’s weight-related behaviors, sticking to a structured reinforcement system, and using behavior change strategies emphasizing warm and positive parentchild interactions (i.e., increasing praise and positive reinforcement, decreasing reliance on negative reinforcement or punishment). The present study examined whether baseline levels and changes in maternal and paternal parenting styles were related to children’s weight loss over 12 months.
Research Methods and Procedures Participants Obese 8- to 12-year-old children and their parents were recruited through physician referral, brochures, flyers, and newspaper ads for a study on different approaches to treating pediatric obesity. The specifics of the trial are presented in detail elsewhere (14). Seventy-two of 128 families who were screened met inclusion criteria, and 63 families entered treatment; of these, 51 children completed baseline and 6-month follow-up data on parenting and adherence for both mother and father and are included in the present analyses. Inclusion criteria included child at or above the 85th BMI (kilograms per meter squared) percentile, one parent willing to attend treatment meetings with the child, 1750
OBESITY RESEARCH Vol. 13 No. 10 October 2005
Table 1. SD)
Sample characteristics (ratio or mean ⫾
Demographics Gender (male/female) Age BMI (kg/m2) Percentage overweight
Child
Mother
Father
18/32 10.0 ⫾ 1.3 41.4 ⫾ 5.3 43.1 ⫾ 6.9 27.8 ⫾ 2.6 29.8 ⫾ 6.3 30.4 ⫾ 5.4 64.7 ⫾ 14.2 38.8 ⫾ 29.2 31.8 ⫾ 23.3
no family members in other weight control programs, no child or parent with psychiatric disorders or dietary or activity restrictions, and child could complete self-monitoring. Analyses showed that the families that were included in the analyses did not differ from the other 12 on baseline child or parent age or percentage overweight, child gender, or any of the baseline parenting scores. One family was eliminated from analyses because it was a statistical outlier and biased the results (as defined below). Characteristics of the final sample are presented in Table 1. The Social and Behavioral Sciences Institutional Review Board of the University at Buffalo approved this study, children provided written assent, and parents provided written consent to participate. Design and Procedures The larger study (14) was designed to compare treatments that differed in the behavioral strategy used to reduce sedentary behaviors. Families in each cohort were randomized into one of two treatment groups: reinforced reduced sedentary behavior or stimulus control of sedentary behaviors. Data were collected at baseline and 6 and 12 months after randomization. Results showed no differences in rate of percentage overweight change between the two groups at 6 or 12 months after randomization, with both groups significantly below baseline. Supplemental analyses showed that subjects who increased physical activity when sedentary behaviors were reduced had larger percentage overweight changes at 6 and 12 months than youth who did not increase their physical activity when sedentary behaviors were reduced. In addition, youth who reduced their intake of lownutrient-dense foods when sedentary behaviors were reduced had greater percentage overweight reductions after 6 months than youth who did not reduce intake of lownutrient-dense foods when sedentary behaviors were reduced (14). The treatment included 20 meetings over the first 6 months. Families were weighed at each session, met with an individual therapist for 15 to 30 minutes, and attended separate 30-minute child and parent classes. The dietary intervention was implemented using the Traffic Light Diet, in which foods are divided into red, yellow, and green
Parenting Style and Child Weight Loss, Stein et al.
classifications based on high, moderate, and low fat and sugar content of foods (1), and behavioral components of treatment included self-monitoring, praise, contracting, preplanning, and problem solving. Participants were provided general information on lifestyle and aerobic activities, but participants were not provided with a specific activity program, and specific goals were not set. All participants were instructed to reduce hours of targeted sedentary activity to 15 or fewer per week. Children in the reinforcement group were provided praise and points for reducing their sedentary behaviors to no more than 15 hours per week, whereas children in the stimulus control group were reinforced for recording their sedentary behaviors but not for behavior change. The children in the stimulus control group were also instructed to change their environment to prevent them from engaging in the targeted behaviors and to establish rules regarding the sedentary behaviors (e.g., homework has to be done before television can be watched) and modifying the television watching environment. Measurements Body Composition. Height was measured in one-eighth inches using a stadiometer (Seca, Columbia, MD), and weight was measured in one-quarter pounds using a medical balance beam scale (Healthometer, Bridgeview, IL), calibrated daily using a 50-pound calibration weight (Troemner, Philadelphia, PA). Percentage overweight was based on comparisons of the BMI with the 50th percentile BMI for age and sex using the Centers for Disease Control growth charts (15). For eight families, 1-year measurements of weight and child height were self-reported and adjusted for self-report bias using laboratory specific regression models based on over 1000 self-reported and measured weight and heights when families were unable to attend assessments. Activity. Participating parents and children recorded any sedentary or physical activity that took 10 minutes or longer in duration. Activity was recorded on index cards, structured with columns for start and stop times and the activity description, over 4 days (2 weekdays and 2 weekend days). The index cards were reviewed in person within a few days of recording to address ambiguous activities or large time gaps. The multiples of resting metabolic rate values for each activity were recorded using the Compendium of Physical Activity (16), and the percentage of time spent in activities that were at least three multiples of resting metabolic rate (considered moderate to vigorous physical activity) (17) was coded (for details on compliance and validation of these data, see 14). Dietary Intake. Dietary intake was measured using a food intake questionnaire (18) designed to assess servings of RED (high energy dense) foods and fruits and vegetables. This questionnaire has been validated against previous day 24-hour recalls (18). Previous research has shown that
changes in RED food intake are related to weight loss (19,20). Adherence. Adherence was measured using a 25-item laboratory-constructed questionnaire to assess maintenance of the behaviors related to weight control learned during the program. Subjects rated the frequency of occurrence of each behavior listed on a five-point scale (1, never; 2, seldom; 3, frequently; 4, almost always; 5, always). Socioeconomic Status. The Hollingshead Four Factor Index was used to measure socioeconomic status before treatment (21). Parenting. The 56-item version (22) of the Child’s Report of Parental Behavior Inventory (CRPBI)1 (23) was used to measure child-rearing behaviors. The CRPBI is a questionnaire that assesses three factors of parenting: acceptance vs. rejection, psychological control vs. autonomy, and firm vs. lax control. Responses are given on a threepoint scale, indicating whether an item is like, somewhat like, or not like the parent. Children complete the 56 items separately for their father’s and mother’s parenting behaviors. The three factors have been found previously in samples of children (24) and college students (25). The scale has strong internal consistency and discriminative validity (23,26). Analytic Strategy ANOVA was used to examine changes in body weight and parenting over time, with group as the between-factor and time as the within-factor. Zero-order Pearson correlations were used to determine the relation of baseline parenting and change in parenting with child’s weight loss maintenance. Hierarchical regression analyses were used to examine the incremental effect of adding parenting as a predictor of child weight control beyond demographics and behaviors that were targeted during the behavioral intervention (i.e., eating, physical activity, and compliance with other program behaviors such as self-monitoring and preplanning). Variables that were significant zero-order predictors of child weight control were included in the hierarchical regression model. The hierarchical regression model included demographics and treatment group in the first step, and measures of eating (change in consumption of RED foods), physical activity (change in percentage of time in moderate to vigorous physical activity), and other program behaviors (e.g., score on the adherence questionnaire) were added in the second step. Baseline parenting factors that were significant were added in the third step, and change in parenting factors, including interactions between significant parenting factors, was added in the fourth step. Baseline levels of any significant change in parenting factor were included in the third step to control for baseline levels. Outliers were iden-
1
Nonstandard abbreviations: CRPBI, Child’s Report of Parental Behavior Inventory.
OBESITY RESEARCH Vol. 13 No. 10 October 2005
1751
Parenting Style and Child Weight Loss, Stein et al.
tified, based on leverage and Studentized residuals, as cases where a Student’s t value for the residual appears that should occur in ⬍1% of the data (27).
Table 3. Pearson product moment correlations between parenting at baseline and change in parenting at 6 months with 12-month changes in child percentage overweight
Results Child percentage overweight changed significantly over time [F(2,96) ⫽ 91.58, p ⬍ 0.001], with child’s percentage overweight significantly decreasing from baseline (64.7 ⫾ 14.2) to 6 months [48.4 ⫾ 17.2; F(1,48) ⫽ 92.58, p ⬍ 0.001] and baseline to 1-year follow-ups [53.6 ⫾ 19.2; F(1,48) ⫽ 27.43, p ⬍ 0.001]. The group-by-time interaction was not significant [F(2,96) ⫽ 0.22, p ⫽ 0.806]. Child report of parenting behaviors is reported in Table 2. Significant changes were observed for father [F(1,48) ⫽ 15.93, p ⬍ 0.001] and mother [F(1,48) ⫽ 4.41, p ⬍ 0.05] acceptance vs. rejection. Mothers and fathers did not change significantly on the other two parenting factors, and there were no significant group-by-time interactions for any of the parenting factors for either mothers or fathers. The relation between baseline parenting or changes in parenting and change in child percentage overweight at 12 months is shown in Table 3. There were no significant baseline parenting predictors of child percentage overweight change, but there was a significant negative correlation (r ⫽ ⫺0.40, p ⫽ 0.004) between father’s change on the first parenting factor (acceptance vs. rejection) and
Table 2. Parenting at baseline and change over 6 months (mean ⫾ SD)
Father Acceptance vs. rejection† Psychological autonomy vs. psychological control Firm control vs. lax control Mother Acceptance vs. rejection* Psychological autonomy vs. psychological control Firm control vs. lax control
Baseline
0 to 6 month ⌬
2.49 ⫾ 0.38
⫺0.16 ⫾ 0.28
1.68 ⫾ 0.49
⫺0.02 ⫾ 0.44
1.46 ⫾ 0.41
⫺0.04 ⫾ 0.35
2.60 ⫾ 0.31
⫺0.07 ⫾ 0.25
1.69 ⫾ 0.40
0.01 ⫾ 0.37
1.47 ⫾ 0.30
⫺0.02 ⫾ 0.32
* Main effect of time, p ⬍ 0.05. † Main effect of time, p ⬍ 0.001.
1752
OBESITY RESEARCH Vol. 13 No. 10 October 2005
Baseline Father’s parenting Acceptance vs. rejection Psychological autonomy vs. psychological control Firm control vs. lax control Mother’s parenting Acceptance vs. rejection Psychological autonomy vs. psychological control Firm control vs. lax control
0.16
0- to 6 month change ⫺0.40*
⫺0.26 ⫺0.10
0.15 0.01
0.05
⫺0.19
⫺0.12 0.01
⫺0.21 ⫺0.06
* p ⬍ 0.01.
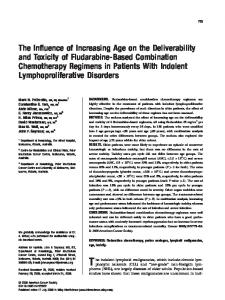
child’s percentage overweight change. The more accepting the father became, the more the child’s percentage overweight decreased. No significant correlations were found with the father’s other parenting factors or with any of the mother’s parenting factors. The hierarchical regression is shown in Table 4. Demographic variables did not significantly predict child percentage overweight change, whereas knowledge of adherence in the second step of the model was a significant predictor which significantly increased the variance accounted for [R2 change ⫽ 0.108, F(1,43) ⫽ 5.81, p ⬍ 0.01]. Baseline father acceptance added to the third step for control purposes, because there were no significant zero-order baseline parenting variables, accounted for additional variance in the model [R2 change ⫽ 0.109, F(1,42) ⫽ 6.64, p ⬍ 0.01]. The addition of other variables in the model may have acted as suppressor variables to increase the strength of the relationship of baseline father acceptance on the primary outcome. Change in father’s acceptance added in step four significantly increased the variance accounted for [R2 change ⫽ 0.096, F(1,41) ⫽ 6.63, p ⬍ 0.01]. The complete model accounted for 43.3% of the variance in child percentage overweight change (p ⫽ 0.004). ANOVA showed differences in the rate of change in percentage overweight for youth who had a father who maintained or increased acceptance (N ⫽ 16) vs. a father who decreased acceptance [N ⫽ 34, F(2,96) ⫽ 7.02, p ⬍ 0.001]. Linear contrasts showed that youth whose fathers increased acceptance had significantly greater percentage overweight decrease from baseline than youth whose fathers decreased acceptance at 6 [⫺19.8 vs. ⫺14.6; F(1,48) ⫽ 4.50, p ⫽ 0.039] and 12 [F(1,48) ⫽ 9.81, p ⫽ 0.003] months (Figure 1).
Parenting Style and Child Weight Loss, Stein et al.
Table 4. Hierarchical regression analysis for 1-year change in child percentage overweight Variables Step 1: demographics Child age Child baseline overweight (%) Child sex Treatment group Socieconomic status Step 2: Change in activity, eating, and adherence Child adherence Step 3: baseline parenting Baseline father’s acceptance Step 4: change in parenting ⌬ father’s acceptance
B
SE 

p
0.43 0.18 4.85 ⫺0.54 0.06
1.18 0.11 3.20 3.03 0.14
0.05 0.24 0.22 ⫺0.03 0.07
0.717 0.112 0.137 0.860 0.659
⫺5.31
2.20
⫺0.36
0.020
10.27
4.00
0.37
0.014
⫺13.48
5.24
⫺0.36
0.014
⌬R2
p ⌬R2
0.201
0.108
⬍0.01
0.310
0.109
⬍0.01
0.406
0.096
⬍0.01
R2 0.093
Change represents 0 to 6 change, B and SE  are the  coefficients, and  is the standardized  coefficient.
Discussion The present results show that change in parenting style plays a role in the long-term outcome of family-based behavioral treatments for child obesity. The only parenting variable that was related to child 1-year percentage overweight change was father’s change in acceptance vs. rejection. In hierarchical regression, it was observed that adding change in acceptance improved the prediction of percentage overweight change, even after accounting for demographics, adherence to weight-related behaviors, and baseline father acceptance.
Figure 1: Percentage overweight at 0, 6, and 12 months for youth who perceived that their fathers maintained or increased their acceptance and reduced rejection vs. youth who perceived that their father reduced their acceptance and increased their rejection.
There were small changes in parenting over time, with fathers and mothers showing a significant decrease in acceptance. A decrease in acceptance over time might be expected, as the typical developmental trend is that as children age, they view their parents as increasing in firm control, but also as decreasing their warmth and acceptance (28). Thus, it may be important that 32% of the fathers were perceived as more accepting and less rejecting over time, and these changes were related to treatment success. Fortytwo percent of the mothers were perceived as becoming more accepting and less rejecting, but those perceptions of maternal changes were not related to treatment success. Perhaps the most striking aspect of the parental data was that change in paternal but not maternal parenting style was related to child weight outcome. This was unexpected because a majority of the families (43 of 50 families, or 86%) had the mother as the participating parent, and the mother attended meetings and was involved in the stimulus control and reinforcement goals. Our findings are consistent with previous research indicating that paternal parenting is associated with child functioning in various domains. For example, paternal acceptance has been found to be a predictor of adolescent functioning outside the home (29), and these investigators suggest that mothers may typically be more unconditionally accepting of their child or that the child is more eager to obtain their father’s acceptance (29). A change in father’s acceptance may indicate a home environment in which all family members are supportive of the healthy behavior changes attempted by the participating child. In contrast, fathers who, for example, continue to keep unhealthy foods in the home for themselves yet expect the overweight child to resist eating them could be seen as OBESITY RESEARCH Vol. 13 No. 10 October 2005
1753
Parenting Style and Child Weight Loss, Stein et al.
not supportive of the child in his/her efforts at health behavior changes. Fathers’ increase in acceptance over the treatment period may be especially powerful because it is contrary to the usual developmental trend at this age, which is for children to perceive their parents as less accepting over time (28). The hierarchical regression showed that parenting contributed to children’s outcome above and beyond the aspects of program adherence and other weight-related behaviors that were included in the present model. It is not surprising that child adherence to the eating and activity goals of a pediatric weight control program would be more successful, but the added influence of parenting beyond adherence represents a new way to conceptualize factors that influence pediatric weight control. It does not seem that the influence of adherence to program goals was mediated by increased father acceptance (r ⫽ 0.17, p ⬎ 0.05), but changes in father acceptance may have increased the motivation of the child to change health behaviors, which was not assessed in this study. Parenting was assessed using child ratings of parent behavior. The Child Report of Parental Behavior Inventory has also been adapted to provide parent ratings of themselves and the other parent, and not surprisingly, parents rate themselves as more accepting and more firm than ratings by the other parent or the child (30). In future studies, it would be interesting to obtain parental ratings of themselves and the other parent to provide additional perspectives on parent behavior. Also, assessing the perception of parent behavior from a sibling would provide another youth perspective on parenting. Although the children are likely to be more objective than their parents on parenting, there may be biases to child ratings that may relate to the relationships observed. For example, it may be that the relation found partly reflects that children who are successful in the program are more likely to view their parents in a positive way, regardless of the parents’ actual parenting behaviors. It would also be interesting to compare the three aspects of parenting style assessed by the CRPBI (acceptance, firm control, and psychological control) to other aspects of parenting and the family environment in terms of their effect on outcome. For example, one could examine how important knowledge of parenting strategies (31), an organized family environment (32), or the use of particular strategies such as reinforcement, modeling, and praise (1) are for children’s success at losing and maintaining weight. As research continues to support the hypothesis that parenting makes an important contribution to child weight control, studies are needed to understand how best to enhance components of parenting that are most related to improvements in treatment outcome. Overall, the present findings suggest that parenting is an important factor in children’s adopting successful strategies to control their weight. Future interventions 1754
OBESITY RESEARCH Vol. 13 No. 10 October 2005
should be enhanced by an even stronger emphasis on positive parenting strategies that communicate acceptance of the child.
Acknowledgment We thank Suzanne Wright for comments on an earlier version of the manuscript. This work was supported by National Institute of Child Health and Human Development Grant R01 HD 39778 (L.H.E.). References 1. Epstein LH, Myers MD, Raynor HA, Saelens BE. Treatment of pediatric obesity. Pediatrics. 1998;101:554 –70. 2. Epstein LH, McKenzie SJ, Valoski A, Klein KR, Wing RR. Effects of mastery criteria and contingent reinforcement for family-based child weight control. Addict Behav. 1994;19: 135– 45. 3. Israel AC, Stolmaker L, Andrian CA. The effects of training parents in general child management skills on a behavioral weight loss program for children. Behav Ther. 1985;16:169 – 80. 4. Israel AC, Stolmaker L, Sharp JP, Silverman WK, Simon LG. An evaluation of two methods of parental involvement in treating obese children. Behav Ther. 1984;15:266 –72. 5. Epstein LH, Roemmich JN, Raynor HA. Behavioral therapy in the treatment of pediatric obesity. In: Styne D, ed. Pediatric Clinics of North America. Philadelphia, PA: W.B. Saunders; 2001, pp. 981–993. 6. Epstein LH, Valoski A, Wing RR, McCurley J. Ten-year follow-up of behavioral family-based treatment for obese children. JAMA. 1990;264:2519 –23. 7. Aragona J, Cassady J, Drabman RS. Treating overweight children through parental training and contingency contracting. J Appl Behav Anal. 1975;8:269 –78. 8. Golan M, Weizman A, Apter A, Fainaru M. Parents as exclusive agents of change in the treatment of childhood obesity. Am J Clin Nutr. 1998;67:1130 –5. 9. Epstein LH, Wisniewski L, Weng R. Child and parent psychological problems influence child weight control. Obes Res. 1994;2:509 –15. 10. Kirschenbaum DS, Harris ES, Tomarken AJ. Effects of parental involvement in behavioral weight loss therapy for preadolescents. Behav Ther. 1984;15:485–500. 11. Davis CL, Delamater AM, Shaw KH, et al. Parenting styles, regimen adherence, and glycemic control in 4- to 10-year-old children with diabetes. J Pediatr Psychol. 2001;26:123–9. 12. Baumrind D. The influence of parenting style on adolescent competence and substance use. J Early Adolesc. 1991;11:56 – 95. 13. Lamborn SD, Mounts NS, Steinberg L, Dornbusch SM. Patterns of competence and adjustment among adolescents from authoritative, authoritarian, indulgent, and neglectful families. Child Dev. 1991;62:1049 – 65. 14. Epstein LH, Paluch RA, Kilanowski CK, Raynor HA. The effect of reinforcement or stimulus control to reduce sedentary behavior in the treatment of pediatric obesity. Health Psychol. 2004;23:371– 80.
Parenting Style and Child Weight Loss, Stein et al.
15. Must A, Dallal GE, Dietz WH. Reference data for obesity: 85th and 95th percentiles of body mass index (wt/ht2) and triceps skinfold thickness. Am J Clin Nutr. 1991;53:839 – 46. 16. Ainsworth BE, Haskell WL, Whitt MC, et al. Compendium of physical activities: an update of activity codes and MET intensities. Med Sci Sports Exerc. 2000;32:S498 –504. 17. Pate RR, Pratt M, Blair SN, et al. Physical activity and public health: a recommendation from the Centers for Disease Control and Prevention and the American College of Sports Medicine. JAMA. 1995;273:402–7. 18. Epstein LH, Gordy CC, Raynor HA, Beddome M, Kilanowski CK, Paluch RA. Increasing fruit and vegetable and decreasing fat and sugar intake in families at risk for childhood obesity. Obes Res. 2001;9:171–9. 19. Epstein LH, Wing RR, Koeske R, Andrasik F, Ossip DJ. Child and parent weight loss in family-based behavior modification programs. J Consult Clin Psychol. 1981;49:674 – 85. 20. Epstein LH. Development of evidence-based treatments for pediatric obesity. In: Kazdin AE, Weisz JR, eds. EvidenceBased Psychotherapies for Children and Adolescents. New York: Guilford Publications, Inc.; 2003, pp. 374 –388. 21. Hollingshead AB. Four Factor Index of Social Status. New Haven, CT; Yale University, 1975. 22. Margolies PJ, Weintraub S. The revised 56-item CRPBI as a research instrument: Reliability and factor structure. J Clin Psychol. 1977;33:472– 6. 23. Schaefer ES. Children’s reports of parental behavior: an inventory. Child Dev. 1965;36:413–24.
24. Armentrout JA, Burger GK. Factor analyses of college students’ recall of parental childrearing behaviors. J Genet Psychol. 1972;121:155– 61. 25. Armentrout JA, Burger GK. Children’s reports of parental child-rearing behavior at five grade levels. Dev Psychol. 1972; 7:44 – 8. 26. Locke LM, Prinz RJ. Measurement of parental discipline and nurturance. Clin Psychol Rev. 2002;22:895–929. 27. Wilkinson L, Blank G, Gruber C. Desktop Data Analysis with SYSTAT. Upper Saddle River, NJ: Prentice Hall; 1996. 28. Burger GK, Lamp RE, Rogers D. Developmental trends in children’s perceptions of parental child-rearing behavior. Dev Psychol. 1975;11:391. 29. Forehand R, Nousiainen S. Maternal and paternal parenting: critical dimensions in adolescent functioning. J Fam Psychol. 1993;7:213–21. 30. Schwarz JC, Barton-Henry ML, Pruzinsky T. Assessing child-rearing behaviors: a comparison of ratings made by mother, father, child, and sibling on the CRPBI. Child Dev. 1985;56:462–79. 31. O’Dell SL, Tarler-Benlolo L, Flynn JM. An instrument to measure knowledge of behavioral principles as applied to children. J Behav Ther Exp Psychiatry. 1979;10:29 –34. 32. Moos RH. Conceptual and empirical approaches to developing family-based assessment procedures: resolving the case of the Family Environment Scale. Fam Process. 1990;29:199 – 208.
OBESITY RESEARCH Vol. 13 No. 10 October 2005
1755