Jun 12, 2013 - motor tasks in children with incomplete spinal cord injuries (ISCIs) .... (MVA), surgical resection secondary to tumor (Tumor Rsx), and transverse ...
J Neurophysiol 110: 1415–1425, 2013. First published June 12, 2013; doi:10.1152/jn.00676.2012.
Modular control of varied locomotor tasks in children with incomplete spinal cord injuries Emily J. Fox,1,2 Nicole J. Tester,1,3 Steven A. Kautz,4,5 Dena R. Howland,6,7 David J. Clark,3 Cyndi Garvan,8 and Andrea L. Behrman6,7 1
Department of Physical Therapy, University of Florida, Gainesville, Florida; 2Brooks Rehabilitation Clinical Research Center, Brooks Rehabilitation, Jacksonville, Florida; 3Brain Rehabilitation Research Center, Malcom Randall Veterans Affairs Medical Center, Gainesville, Florida; 4Department of Health Sciences and Research, Medical University of South Carolina, Charleston, South Carolina; 5Center for Rehabilitation Research in Neurological Conditions, Medical University of South Carolina, Charleston, South Carolina; 6Department of Neurological Surgery, University of Louisville, Louisville, Kentucky; 7Kentucky Spinal Cord Injury Research Center, University of Louisville, Louisville, Kentucky; and 8Office of Educational Research, University of Florida, Gainesville, Florida Submitted 3 August 2012; accepted in final form 11 June 2013
Fox EJ, Tester NJ, Kautz SA, Howland DR, Clark DJ, Garvan C, Behrman AL. Modular control of varied locomotor tasks in children with incomplete spinal cord injuries. J Neurophysiol 110: 1415–1425, 2013. First published June 12, 2013; doi:10.1152/jn.00676.2012.—A module is a functional unit of the nervous system that specifies functionally relevant patterns of muscle activation. In adults, four to five modules account for muscle activation during walking. Neurological injury alters modular control and is associated with walking impairments. The effect of neurological injury on modular control in children is unknown and may differ from adults due to their immature and developing nervous systems. We examined modular control of locomotor tasks in children with incomplete spinal cord injuries (ISCIs) and control children. Five controls (8.6 ⫾ 2.7 yr of age) and five children with ISCIs (8.6 ⫾ 3.7 yr of age performed treadmill walking, overground walking, pedaling, supine lower extremity flexion/extension, stair climbing, and crawling. Electromyograms (EMGs) were recorded in bilateral leg muscles. Nonnegative matrix factorization was applied, and the minimum number of modules required to achieve 90% of the “variance accounted for” (VAF) was calculated. On average, 3.5 modules explained muscle activation in the controls, whereas 2.4 modules were required in the children with ISCIs. To determine if control is similar across tasks, the module weightings identified from treadmill walking were used to reconstruct the EMGs from each of the other tasks. This resulted in VAF values exceeding 86% for each child and each locomotor task. Our results suggest that 1) modularity is constrained in children with ISCIs and 2) for each child, similar neural control mechanisms are used across locomotor tasks. These findings suggest that interventions that activate the neuromuscular system to enhance walking also may influence the control of other locomotor tasks. locomotion; module; spinal cord injury; synergies; walking
are fundamental for the control of a variety of locomotor behaviors (Calancie et al. 1994; Dimitrijevic et al. 1998; Dobkin et al. 1995; Grillner 1979; Grillner and Zangger 1975; Grillner et al. 2008; Marder and Bucher 2001; Nadeau et al. 2010; Rossignol et al. 2006). Furthermore, studies of animal locomotion indicate that neural networks that are fundamental in controlling a variety of locomotor behaviors may overlap, thereby resulting in shared control during tasks
SPINAL NEURAL NETWORKS
Address for reprint requests and other correspondence: E. J. Fox, Dept. of Physical Therapy, Univ. of Florida, Gainesville, FL 32610 (e-mail: ejfox @phhp.ufl.edu). www.jn.org
such as stepping, swimming, and galloping (Berkowitz 2008; Earhart and Stein 2000; Forssberg et al. 1980; Mortin and Stein 1989). In humans, evidence of consistent muscle timing and interlimb coordination across varied tasks also suggests neural mechanisms used to control a variety of locomotor tasks may be similar (Lamb and Yang 2000; Patrick et al. 2008; Wannier et al. 2001; Zehr 2005; Zehr et al. 2007). The complexity of controlling an extensive repertoire of locomotor tasks may be simplified by the nervous system using a dimensional reduction strategy, in which a limited set of modules is recruited and flexibly combined to control a variety of tasks (Bizzi et al. 1991, 2000, 2008; Dominici et al. 2011; Hart and Giszter 2010; Ivanenko et al. 2004, 2005; Kargo and Giszter 2000; Mussa-Ivaldi et al. 1994; Ting 2007; Ting and Macpherson 2005; Tresch et al. 1999). A module is a functional unit of the nervous system, largely controlled by brain stem and spinal neural networks (Hart and Giszter 2010; Roh et al. 2011), that specifies functionally relevant patterns of muscle activation (Dominici et al. 2011). The selection and timing of modular activation is dependent on task biomechanics (Clark et al. 2010; Ivanenko et al. 2003; McGowan et al. 2010; Neptune et al. 2009; Ting and Macpherson 2005) and sensory feedback (Cheung et al. 2005; Kargo and Giszter 2008). Cortical activation also may influence modular control (Gentner and Classen 2006; Holdefer and Miller 2002; Kozlov et al. 2009). Adult human locomotion can be explained by a set of four to five modules, identified using computational algorithms applied to multiple electromyogram (EMG) recordings (Clark et al. 2010; Dominici 2011; Ivanenko et al. 2004, 2005). Modular output is associated with biomechanical features of walking and remains consistent even when factors such as gait speed and body weight support are varied (Clark et al. 2010; Ivanenko et al. 2004). Furthermore, modular output associated with walking can explain muscle activation during other locomotor tasks such as recumbent stepping and arm and leg cycling (Stoloff et al. 2007; Zehr et al. 2007). Similar modular control across locomotor tasks further suggests the underlying neural mechanisms are similar (d’Avella et al. 2003; Tresch et al. 1999). Examination of modular control not only provides insight into the mechanisms underlying locomotor control but also 1415
1416
MODULAR CONTROL OF LOCOMOTION IN CHILDREN
provides information regarding the effects of neurological injuries (Cheung et al. 2012; Safavynia et al. 2011). For example, adults poststroke exhibit fewer modules during walking, and this constraint on modular output is associated with decreased gait speed (Bowden et al. 2010; Clark et al. 2010) and poor biomechanical control (Clark et al. 2010). Similarly, adults with ISCIs express fewer modules during walking (Hayes et al. 2011), and the modules are characterized by greater coactivation of antagonistic muscles (Fox et al. 2011; Hayes et al. 2011). Although evidence has emerged regarding the effects of neurological injuries on modular control in adults, the impact of neurological injury on locomotor control mechanisms in children is not well understood (Behrman et al. 2008; Damiano and DeJong 2009; Vogel and Lubicky 1995). The effects of ISCI on modular control mechanisms in children may differ substantially due to their immature and developing nervous systems (Bregman and Goldberger 1983; Dominici et al. 2011; Petersen et al. 2010). Preliminary evidence of the mechanisms underlying locomotor control in children emerged in our case report of a child with severe ISCI (Behrman et al. 2008). This child recovered reciprocal leg movements enabling independent ambulation with a rolling walker following 76 sessions of locomotor training (Behrman et al. 2008). Interestingly, the child also used similar leg movements to perform other locomotor tasks such as crawling, stair climbing, and tricycle pedaling. The child, who was injured at 3.5 yr of age, could not perform these tasks after his ISCI and did not practice them; they emerged following his participation in locomotor training and recovery of reciprocal stepping (Fox et al. 2010). Based on evidence of neural control strategies used across locomotor tasks, this observation suggests that children may use similar neural mechanisms to control a variety of locomotor tasks and that these mechanisms may persist following ISCI. The purpose of this study, therefore, was to examine neuromuscular control of reciprocal locomotor tasks (treadmill walking, overground walking, stair climbing, tricycle pedaling,
crawling, and supine lower extremity flexion and extension) in children with ISCIs as well as children without neurological injuries (controls). We hypothesized that compared with controls, children with ISCIs would utilize fewer modules to control varied locomotor tasks, suggesting that modules may not be independently activated after neurological injury (Clark et al. 2010). Additionally, we hypothesized that each child’s (controls and children with ISCIs) pattern of muscle activation would be similar across the varied locomotor tasks, indicating a consistent modular control strategy was used across the tasks. METHODS
Participants Five children with intact nervous systems (controls) and five children with ISCIs, classified by the American Spinal Injury Association (ASIA) Impairment Scale as “C” (motor incomplete), participated. The children with ISCIs were injured for ⬎1 yr. All children were 3–13 yr old (Table 1). This age range was selected because a mature gait pattern typically develops by 3 yr (Sutherland et al. 1980). All children were free from musculoskeletal impairments or secondary health conditions. Inclusion criteria for the children with ISCIs included clinical signs of central nervous system injury such as ankle clonus or positive Babinski reflex. Medical approval for participation was obtained for all children with ISCIs. All study procedures were approved by the University of Florida Institutional Review Board; parents provided written informed consent, and each child provided their assent to participate in the study. General Procedures Each child with ISCI was examined according to the ASIA International Standards for Neurological and Functional Classification of Spinal Cord Injury (American Spinal Injury Association 2006). The severity of each child’s injury was classified based on the ASIA Impairment Scale and volitional lower extremity movement was assessed using the Lower Extremity Motor Score (Table 1) (American Spinal Injury Association 2006). Lower extremity EMGs were recorded during a variety of rhythmic, reciprocal locomotor and loco-
Table 1. Subject demographics and task participation for controls and children with ISCIs Subject
Age, yr
C-1 C-2 C-3 C-4 C-5 (F) Avg. SD SCI-1 SCI-4 SCI-5 SCI-6 SCI-7 Avg. SD
9 6 7 13 8 9 4 9 12 7 12 3 9 3
Injury Level
C7 T4–T8 C4-7 T10 C1–T6
Age of Injury, yr
Etiology
GSW Tumor Rsx Unknown* MVA Tr. myelitis
3.5 8.5 6 mo 10.5 5 mo
LEMS
4/50 0/50* 4/50 0/50* 0/50*
OG Gait Speed, m/s
TM Speed, m/s
0.88 1.21 2.03 0.81 0.90 1.17 0.51 0.57
0.78 0.78 0.72 0.72 0.33 0.67 0.19 0.56 0.58 0.83 0.64 0.89 0.70 0.15
0.36 0.47 0.15
Pedaling
Supine Flex/Ex
X X X X X
X X X X X
X X X X X
X X X X X
Stair Climbing
Crawling
X X
X X X X X
X X
X X X
Data indicate demographics and task participation for controls (C) or children with incomplete spinal cord injuries (ISCIs); 1 female (F) subject participated. Etiologies of the SCIs are reported as gunshot wound (GSW), unknown *, or unknown but suspected cause of transverse myelitis or trauma secondary to motor vehicle accident (MVA), surgical resection secondary to tumor (Tumor Rsx), and transverse myelitis (Tr. myelitis). Ages are reported in years unless otherwise indicated. The Lower Extremity Motor Score (LEMS) is based on voluntary isolated joint movements and strength in 5 bilateral muscles; asterisks indicate an inability to perform isolated joint movements in the standardized position (American Spinal Injury Association 2006). Overground (OG) and treadmill (TM) walking speeds are reported: X indicates the child performed the task indicated [pedaling; supine lower extremity flexion/extension (supine flex/ex), stair climbing, and crawling]; no value indicates the task was not performed or electromyograms (EMGs) were not usable. Average (Avg.) and SD values are reported for controls and children with ISCIs. J Neurophysiol • doi:10.1152/jn.00676.2012 • www.jn.org
MODULAR CONTROL OF LOCOMOTION IN CHILDREN
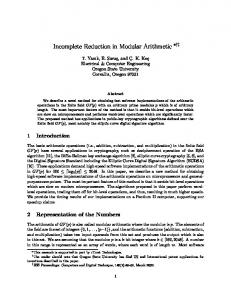
motor-like tasks, which included treadmill walking, overground walking, pedaling, supine lower extremity flexion/extension, stair climbing, and crawling (details provided below). Control children independently performed all tasks, whereas children with ISCIs often required physical assistance (Table 1). Two to three trials of each task were performed. The trials each were 30 – 60 s in duration for treadmill walking, pedaling, and supine flexion/extension. Overground walking and crawling occurred on a 15-ft pathway, and 3– 4 contiguous stairs were used for stair climbing. Each child’s performance of the tasks was monitored for consistency in the timing and amplitude of the movements. Performance details of each locomotor task are provided below. Treadmill walking. After acclimation to treadmill walking, children walked on a 2.5-ft-wide standard treadmill surface (Fig. 1). All children were discouraged from holding onto the rails and were encouraged to swing their arms reciprocally. Children with ISCIs wore a body weight support harness (Robertson Harnesses, Henderson, NV) attached to a fixed overhead support to unweight ⬃40% of their body weight and prevent falls. Body weight support and assistance during treadmill walking were provided in accordance with locomotor training principles and therefore emphasized upright trunk posture, appropriate lower extremity kinematics, and rhythmic stepping with weight bearing on the lower extremities (Behrman and Harkema 2000). All children were encouraged to walk using a normal gait pattern, and treadmill speeds were selected to maintain consistency across children yet account for each child’s ability and comfort level. Overground walking. Controls and ambulatory children with ISCIs (n ⫽ 2) walked independently across a 15-ft walkway at a selfselected comfortable speed. The two children with ISCIs who were able to complete this task used reverse rolling walkers (Fig. 1). Pedaling. Pedaling was performed at a consistent, rhythmic pace using a stationary bicycle or adapted tricycle. As needed, children with ISCIs were assisted to maintain a consistent pace for the duration of each pedaling trial. Children with ISCIs were secured at their waist and chest for safety. Foot straps were used to prevent their feet from slipping off the pedals (Fig. 1). Supine lower extremity flexion/extension. Rhythmic, reciprocal lower extremity flexion and extension, mimicking cycling or stepping movements, was performed in a supine position. Controls were cued to perform consistent, full-range movements. Children with ISCIs received physical assistance to perform full-range lower extremity movements at a consistent pace, for several repetitions (Fig. 1). Stair climbing. Controls (n ⫽ 2) and children with ISCIs (n ⫽ 2) ascended three to four contiguous steps without a railing. The children with ISCIs required physical assistance to maintain upright balance without an assistive device or railing. They independently initiated
1417
reciprocal lower extremity flexion and extension movements to negotiate the stairs (Fig. 1). Crawling. Crawling was performed in a standard quadruped position using a consistent, reciprocating movement pattern (Fig. 1). Children with ISCIs were manually cued to maintain trunk alignment (e.g., tactile cues to not arch or extend their lumbar spine) and to appropriately place their hands and lower extremities during crawling. Data Acquisition To obtain overground gait speed and identify cycles of locomotor activity, children were instrumented with reflective markers using the modified Helen Hayes marker set (Kadaba et al. 1989). Kinematic data were acquired with an eight-camera passive motion analysis system (Vicon Motion Systems, Oxford, UK). EMG data were recorded during all locomotor tasks using silver-silver chloride surface electrodes placed bilaterally on lower extremity muscles: tibialis anterior (TA), medial gastrocnemius (MG), vastus medialis (VM), rectus femoris (RF), medial hamstrings (MH), and gluteus medius (GM). Electrodes were placed longitudinally over the muscle belly with an interelectrode distance of ⬃2.0 cm. Interelectrode distance was decreased for smaller children to minimize cross talk (Winter et. al. 1994), and electrodes and leads were secured with tape and medical wrap to prevent mechanical artifact. EMG data were acquired using a synchronized telemetry system (Konigsberg Instruments, Pasadena, CA), sampled at ⱖ1,200 Hz using Vicon software, and saved to disk for off-line analysis. Data Analysis Data were analyzed using custom-written Matlab (The MathWorks, Natick, MA) programs. Overground gait speed was calculated on the basis of the sagittal plane excursion of a reflective marker affixed to a bony landmark on the child’s trunk, e.g., C-7 spinous process. Cycles of locomotor activity (e.g., gait cycles, crawling cycles) were determined by visual inspection of the trajectory of the reflective markers affixed to the child’s lower extremities. Specifically, kinematic data were viewed frame by frame, and cycle initiation was consistently defined as initial contact of the lower extremity (foot or knee, according to the task) to the next consecutive contact of the same limb during treadmill walking, overground walking, stair climbing, and crawling. In a similar manner, cycles of pedaling and supine lower extremity flexion/extension were defined by each revolution of the lower extremity, starting with the initiation of extension motion of the lower extremity to the next subsequent onset of limb extension. Thus each lower extremity completed cycles of locomotor activity
Fig. 1. Children with incomplete spinal cord injuries (ISCI) performing locomotor tasks: treadmill walking, overground walking, supine flexion/extension, tricycle pedaling, crawling, and stair climbing.
J Neurophysiol • doi:10.1152/jn.00676.2012 • www.jn.org
1418
MODULAR CONTROL OF LOCOMOTION IN CHILDREN
defined by active limb extension [e.g., pushing downward during pedaling or weight bearing (stance) during walking] and limb flexion (e.g., initial forward progression during the swing phase of gait). EMG data were high-pass filtered at 30 Hz with a zero-lag fourthorder Butterworth filter, demeaned, rectified, and smoothed with a zero-lag fourth-order 4-Hz low-pass Butterworth filter. To minimize the influence of large variations in activation magnitude across muscles, EMG data for each muscle were normalized to that muscle’s mean value during that trial. Data were resampled at each 1% of the activity cycle and divided into two regions: flexion or extension phase of locomotor activity. Nonnegative matrix factorization. For each subject and each lower extremity, the original EMG data (EMGo) for each trial of locomotor activity were combined into an m ⫻ t matrix, where m is the number of muscles (maximum ⫽ 6 muscles) and t is the time [t ⫽ number of cycles of activity ⫻ 101 (i.e., 0 –100% of the activity cycle)]. A nonnegative matrix factorization (NNMF) algorithm (Lee and Seung 1999; Ting and Macpherson 2005) was applied to the original m ⫻ t matrix. After the number of modules (n) is specified, the NNMF algorithm iteratively populates two matrices. Matrix 1 (m ⫻ n) indicates the relative weighting of each muscle within each module. The NNMF algorithm permits muscles to belong to more than one module, and the weighting for each muscle is held constant across the gait cycle. Matrix 2 (n ⫻ t) indicates the relative activation magnitude of each module across the gait cycle. The product of these matrices is a reconstruction of the EMG (EMGr). The agreement between EMGr and EMGo was calculated using the sum of the squared errors: (EMGo ⫺ EMGr)2. The NNMF algorithm iteratively adjusts matrix 1 and matrix 2 until the error between EMGo and EMGr is minimized. Determining the number of modules to reconstruct the original EMG data. To determine how well EMGr explained the variability in the EMGo, the variance accounted for (VAF) was calculated separately for each leg and locomotor task, for each subject (Eq. 1). VAF values also were calculated separately for each muscle and gait cycle region to ensure a high integrity of reconstruction. VAF ⫽ 1 ⫺ (EMGo ⫺ EMGr) ⁄ 2
EMG2o
(1)
The reconstructed models and VAF values were calculated and compared using one, two, three, four, and five modules. The number of modules required to adequately reconstruct the EMG data was defined as the smallest number of modules for which the overall VAF was ⱖ90% and the VAF for each individual muscle and region of the locomotor cycle (flexion or extension) was ⱖ85% (Clark et al. 2010). In some instances, the overall VAF was ⱖ90% but the VAF values for some muscles and regions of the data were ⬍85%. In these cases, if the addition of another module to the reconstructed model did not
increase the overall VAF more than 4%, the lower number of modules was accepted (Ting and MacPherson 2005). Determination of modular control used across locomotor tasks. To determine whether the muscle groupings that control treadmill walking were activated together in a similar manner for control of overground walking, pedaling, supine flexion/extension, stair climbing, and crawling, the module weightings (i.e., matrix 1) from treadmill walking (for each child) were used to reconstruct the EMG from each of the other locomotor tasks (Gizzi et al. 2011; Torres-Oviedo et al. 2006). That is, NNMF was run for each locomotor condition with matrix 1 fixed at the values obtained from treadmill walking and matrix 2 undergoing the previously described iterative optimization procedure. Statistical Analysis To determine if children with ISCIs use fewer modules to control locomotor tasks, group differences (controls vs. ISCI) in the overall number of modules used across all locomotor tasks were compared using a Wilcoxon rank-sum test. We followed this comparison with a post hoc analysis of our statistical power. Group differences in the number of modules used during each locomotor task also were examined using the Fisher’s exact test. To further determine the difference between the two groups, the effect size was calculated for each locomotor task, using Cohen’s d, based on the pooled standard deviation from both groups. Statistical significance was established at P ⬍ 0.05. The methods described above (Determination of modular control used across locomotor tasks) were used to quantitatively assess if, for each child, the pattern of muscle activation during treadmill walking could account for the pattern of muscle activation used during other locomotor tasks (Gizzi et al. 2011; Torres-Oviedo et al. 2006). RESULTS
Number of Modules Used by Controls and Children With ISCIs Across all locomotor tasks, an average of 3.26 modules (SD ⫽ 0.65; mode ⫽ 3) was required to account for muscle activation in the lower extremities of control children (5 children, n ⫽ 10 lower extremities) (Table 2). Four modules were required in 38% of the cases, three modules in 51% of the cases, and two modules in 11% of the cases (Table 3; Figs. 2 and 3). Across the tasks, crawling required the highest number
Table 2. Average number of modules required for each locomotor task in the two groups of children and average VAF values for the modules identified when the treadmill muscle weights were applied Number of Modules Required to Reconstruct EMG Data
Average VAF Values for Modules Identified Using Treadmill Module Muscle Weightings
Task
Control children
Children with ISCIs
Effect size (Cohen’s d)
Control children
Children with ISCIs
TM walking OG walking Pedaling Supine flex/ex Stair climbing Crawling Avg. Mode
3.40 (0.52) 3.30 (0.48) 3.22 (0.97) 2.90 (0.74) 3.00 (0.00) 3.60 (0.52) 3.26 (0.65) 3.00
2.80 (0.79) 2.00 (0.00)* 1.80 (0.63) 1.70 (0.48) 2.25 (0.50) 2.25 (0.50)* 2.11 (0.71)* 2.00
0.91 5.41 1.77 1.96 3.00 2.64 1.69
92.95 (4.29) 91.85 (4.15) 92.06 (6.46) 86.57 (4.97) 91.42 (6.39) 91.63 (5.29)
94.58 (0.98) 95.29 (3.35) 94.93 (2.30) 90.59 (3.63) 90.66 (4.00) 93.88 (3.37)
Values are means; SD are indicated in parentheses. The number of modules used by children with ISCIs was lower than the number required by control children (*P ⬍ 0.05, 1-sided) overall and for overground walking (*P ⬍ 0.05) and crawling (*P ⬍ 0.05). According to Cohen’s convention (1988), large effect sizes were detected for each of the group comparisons (⬎0.80). Variance accounted for (VAF) indicates the average percentage of the variance accounted for when the muscle activations for treadmill walking were used to reconstruct the EMG data recorded during other locomotor tasks. Values are indicated for TM walking, OG walking, pedaling, supine flexion/extension, stair climbing, and crawling. J Neurophysiol • doi:10.1152/jn.00676.2012 • www.jn.org
MODULAR CONTROL OF LOCOMOTION IN CHILDREN
Table 3. Percentage of lower extremities in each group of children that required 1 to 4 modules to achieve ⱖ90% of the VAF in the EMGs recorded during each locomotor task Controls/ISCIs, %
Task (no. of lower extremities per group)
1 Module
2 Modules
3 Modules
4 Modules
TM walking (10/10) OG walking (10/4) Pedaling (9/10) Supine flex/ex (10/10) Stair climbing (4/4) Crawling (10/4)
0/0 0/0 0/30 0/30 0/0 0/0
0/40 0/100 33/60 30/70 0/75 0/75
60/40 70/0 11/10 50/0 100/25 40/10
40/20 30/0 56/0 20/0 0/0 60/0
For each locomotor task, the number of lower extremities that were included in the calculation is indicated in parentheses for controls and children with ISCIs (Controls/ISCIs). For each group, the percentage of lower extremities that required 1 to 4 modules to achieve ⱖ90% of the VAF in the EMGs recorded during each locomotor task is indicated.
of modules (average of 3.60 modules) and supine flexion/ extension required the fewest modules (average of 2.90 modules) (Tables 2 and 3). Fewer modules were needed to account for muscle activation in the lower extremities of children with ISCIs compared with controls (1-sided, P ⬍ 0.05) (Tables 2 and 3; Fig. 4) when evaluated across all tasks. The statistical power of this group comparison was 0.77. An average of 2.11 modules (SD ⫽ 0.71; mode ⫽ 2) was required to account for the EMG data recorded in lower extremities of children with ISCIs. Four modules were required in 5% of the cases, three modules in 17% of the cases, two modules in 64% of the cases, and one module in 14% of the cases (Table 3). Treadmill walking had the highest module requirement with an average of 2.80 modules. Supine flexion/ extension required the fewest modules, requiring an average of 1.70 modules (Tables 2 and 3). Module Composition and Timing of Activation The modules exhibited by control children during overground and treadmill walking displayed characteristics similar to modules identified in the lower extremities of healthy adults (Clark et al. 2010). In children who required four modules to account for their lower extremity muscle activation during walking, module C-1a, which was active during early stance, consisted primarily of VM and GM activation, and to a lesser extent, RF activation (Fig. 2). Module C-2a consisted mainly of MG activation and was active during late stance. Module C-3a was composed of TA and RF activation and was active during early swing and late swing to early stance. Module C-4a was active during late swing to early stance and consisted of MH activation, and to a lesser extent, TA activation (Fig. 2). In children who required three modules to account for their lower extremity muscle activation during walking (Fig. 3), two of the modules had characteristics similar to the modules in the four-module set, and one module exhibited characteristics of combined module activation. Module C-1b had characteristics of modules C-1a and C-2a (Fig. 3). This was apparent based on dual peaks in the activation timing profile (peaks in early and late stance) and representation of VM and RF (generally seen in early stance, module C-1a) combined with representation from MG (active during late stance, module C-2a). Module C-2b displayed attributes of module C-3a (TA and RF activation during early to mid swing), and module C-3b exhibited
1419
properties similar to module C-4a (identified in the 4-module set) (Fig. 3). In contrast to the task-specific activation timing observed in the modules identified in controls, the modules identified in the children with ISCIs exhibited coactivation across multiple muscles and less distinct activation timing. This was most apparent in the lower extremities of children who required two modules to account for muscle activation during overground or treadmill walking. Coactivation across nearly all muscles except MH was evident in module SCI-1a (Fig. 4A). This module was active during stance. Distinct from the modules used by controls, this module included substantial coactivation in antagonistic muscles MG and TA. The second module, module SCI-2a, with a single peak of activation during swing, had the highest representation from MH with smaller contributions from the other muscles (Fig. 4A). One child, SCI-6, required four modules to account for his pattern of muscle activation during treadmill stepping. However, this child could not stand or walk overground and could not perform isolated lower extremity joint movements. The representation of muscles within each of the four modules used by this child displayed characteristics similar to those used by controls (Fig. 4B). Module SCI-1b had strong representation from VM and RF, but was active during late stance, rather than early stance. Module SCI-2b consisted of strong representation from the MG; however, timing of the module across the gait cycle was variable. Module SCI-3b had strong representation from the TA and was active during late stance and early swing. The fourth module (module SCI-4b) consisted of MH activation and the peak of activation coincided with mid swing (Fig. 4B). Neuromuscular Control Across Locomotor Tasks With the use of the muscle weightings from treadmill walking and task-specific timing profiles, the VAF exceeded 86% for all locomotor tasks in both groups of children (Table 2). Specifically, for the controls, the VAF was ⬎90% for the tasks of overground walking, pedaling, supine flexion/extension, and crawling. The VAF exceeded 90% for all tasks performed by the children with ISCIs (Table 2). DISCUSSION
The purpose of this study was to examine neuromuscular control of reciprocal locomotor tasks in children with ISCIs as well as uninjured children. Across both groups of children, lower extremity muscle activation during five reciprocal locomotor tasks was explained by a small set of motor modules. The data indicate that fewer modules are used to control locomotor tasks in children with ISCIs. For each child, the pattern of muscle activity evident in the modules during treadmill walking explained a high proportion of the variance (VAF values exceeded 86%) in the EMG data recorded during other reciprocal locomotor tasks. This finding was robust in all children in both groups and is consistent with previous studies in animals (Earhart and Stein 2000; Forssberg et al. 1980) and healthy adults (Stoloff et al. 2007; Wannier et al. 2001; Zehr et al. 2007). Similar modular organization across tasks suggests that the nervous system can construct complex lower extremity movements from a small set of building blocks. Our findings
J Neurophysiol • doi:10.1152/jn.00676.2012 • www.jn.org
1420
MODULAR CONTROL OF LOCOMOTION IN CHILDREN Muscle Weightings
Module Activation Timing Profiles
Module C-1a
Module C-1a: Weight Acceptance
Module C-2a
Module C-2a: Propulsion
Module C-3a
Module C-3a: Ground Clearance
0
1
0
1
Relative module activation levels
Fig. 2. Muscle module weightings and timing profiles for 4 modules identified in control children during overground walking. Left: muscle weightings for the 10 lower extremities are shown for the tibialis anterior (TA), medial gastrocnemius (MG), vastus medialis (VM), rectus femoris (RF), medial hamstrings (MH), and gluteus medius (GM) muscles. Bars represent the relative activation of each muscle in the module. Each bar corresponds to data from 1 lower extremity; the data are sorted from greatest to least for each muscle. The weighting for the muscle with the greatest activation is set to 1. Right: activation timing profiles indicate the relative level of activation of a module across the gait cycle (0 –100%). The timing profiles from 1 representative lower extremity are shown. Each module was active at a distinct time point consistent with key biomechanical demands for overground walking (Clark et al. 2010; Neptune et al. 2009).
Relative muscle weightings within each module (normalized to one)
1
0
Module C-4a
1
0
TA
MG
VM
RF
MH GM
Module C-4a: Leg Deceleration
0
20
40
60
80
100
Gait cycle (%)
indicate that this fundamental control strategy is present both in uninjured children and following pediatric ISCI. Effect of Pediatric ISCI on Modular Control of Locomotor Tasks Consistent with our hypothesis, fewer modules were required to explain the muscle activation in the lower extremities of children with ISCIs performing a variety of rhythmic, reciprocal locomotor tasks compared with healthy, uninjured children. Children with ISCIs most often required two modules and relied on synergistic muscle coactivation across the flexion and extension phases of each task (Fig. 4A). The timing of each module was consistent with the general reciprocating limb movements associated with each task. The coactivation of antagonistic muscles, such as the TA and MG in module SCI-1a during the extension phase of the movement (Fig. 4A), however, was inconsistent with the modules identified in the control children and the task requirements. The use of fewer modules and the timing of activation suggest a less complex coordination strategy in which modules may be coactivated to a greater extent due to damage to neural control structures (Cheung et al. 2012). For instance, based on the pattern of muscle activation and activation timing during the first 50% of the gait cycle, module SCI-1a (Fig. 4A) appears to be coactivation of modules C-1a and C-2a (Fig. 2). Clark et al. (2010)
similarly reported “merged” or co-activated modules in the hemiparetic lower extremities of ambulatory adults poststroke, and the presence of merged modules was associated with walking impairment (Clark et al. 2010). Merging of modules, therefore, may reflect a complex interaction between fundamental control strategies and altered task biomechanics. After ISCI, a reduced number of modules also likely reflects damage to neural control structures or altered neural control (Cheung et al. 2012; Hart and Giszter 2004). Specifically, each task required rhythmic, reciprocal lower extremity flexion and extension movements that are believed to be organized largely by spinal pattern generators located below the level of the SCI lesion (Dietz 2003; Edgerton et al. 2004). These neural centers were not directly damaged in the children with ISCIs, since the lesions were above the lumbosacral region (Table 1). Descending input to these lumbosacral segments, however, likely was disrupted substantially. Basic science studies indicate that reduced descending input results in more extensive muscle coactivation (Hart and Giszter 2004), and this also is evident in adults poststroke (Cheung et al. 2012). This is consistent with the reduced lower extremity motor scores of the children with ISCIs, suggesting corticospinal input was severely compromised. In contrast to these findings in children with ISCIs, control children most often required three or four modules to account
J Neurophysiol • doi:10.1152/jn.00676.2012 • www.jn.org
MODULAR CONTROL OF LOCOMOTION IN CHILDREN
1
Module Activation Timing Profiles
Module C-1b
Module C-1b
Module C-2b
Module C-2b
0
Fig. 3. Muscle module weightings and timing profiles for the 3 modules identified in 1 control child during treadmill walking. Left: muscle weightings for both lower extremities are shown for TA, MG, VM, RF, MH, and GM muscles. Bars represent the relative activation of each muscle in the module. The weighting for the muscle with the greatest activation is set to 1. Right: activation timing profiles indicate the relative level of activation of each module across the gait cycle (0 –100%).
1
Relative module activation levels
Relative muscle weightings within each module (normalized to one)
Muscle Weightings
1421
0
Module C-3b 1
0
TA
MG
VM
RF
MH
GM
Module C-3b
0
20
40
60
80
100
Gait cycle (%)
for muscle activation across varied locomotor tasks. A set of four or five motor modules is required to account for muscle activation during walking in healthy adults (Clark et al. 2010; Ivanenko et al. 2004). The activation timing profiles of the modules used by control children during treadmill and overground walking were highly consistent with modular activation in healthy adults (Clark et al. 2010; Ivanenko et al. 2004; Neptune et al. 2009) and children (Dominici et al. 2011). In the set of three modules, the dual activation timing peaks in module C-1b appeared to be a merging of modules C-1a and C-2a (Fig. 3). Furthermore, the timing of this module during stance was relatively consistent with the timing of module activation identified in healthy preschool children (Dominici et al. 2011). Each of the four modules identified in control children was active in a specific region of the gait cycle that was appropriate for achieving the biomechanical requirements of that region (Fig. 2). This suggests that in the uninjured nervous system, modular organization of muscle activity serves to facilitate specific biomechanical task demands (Neptune et al. 2009; Torres-Oviedo et al. 2006). Modular Organization is Similar Across Varied Locomotor Tasks For both groups, the modular organization of muscle activation defined from treadmill walking explained a high proportion (in nearly all instances ⱖ90%) of the muscle activation used during overground walking, pedaling, supine flexion/ extension, stair climbing and crawling. This finding is consistent with studies of vertebrate locomotion in animal models and recent work in humans (Earhart and Stein 2000; Forssberg et al. 1980; Stoloff et al. 2007; Wannier et al. 2001). Furthermore, basic science studies suggest that similarities in modular
control reflect similar neural control mechanisms used across locomotor tasks (Bizzi et al. 2000; Ting and Macpherson 2005). Thus, overall, our findings are consistent with the notion that the nervous system utilizes a fundamental set of building blocks to construct complex motor behaviors (Bizzi et al. 2008; Cheung et al. 2005). Task-Specific Sensory Input Alters Modular Organization Although all of the locomotor tasks required rhythmic, reciprocal lower extremity movements, each task also had distinctive requirements for joint kinematics, postural stabilization, limb loading, and upper extremity use. Furthermore, the tasks varied in the degree of optic flow and vestibular input. These diverse task demands and afferent inputs may be reflected in the variations in modular control demonstrated across the locomotor tasks. While we did find that the modules for treadmill walking can explain at least 86% of the VAF in the EMG from all other tasks, we also found a consistent order to the ranking of the number of modules required for each task. For instance, on average, supine flexion/extension had the lowest modular requirement across both groups. This task does not require trunk stabilization or lower extremity weight bearing. Moreover, during supine flexion/extension, the hip joint does not move into an extended position (Fig. 1). Limb loading (Harkema et al. 1997) and hip joint position (Dietz et al. 2002) are two critical afferent inputs that influence and modulate motor output during locomotion (Ferris et al. 2004; Maegele et al. 2002). Absence of these locomotor-specific inputs may account for the reduced number of modules required to explain muscle activation during supine flexion/extension. The role of locomotor-specific afferent input also may explain why treadmill walking required the greatest number of
J Neurophysiol • doi:10.1152/jn.00676.2012 • www.jn.org
1422
MODULAR CONTROL OF LOCOMOTION IN CHILDREN Muscle Weightings
A
Module Activation Timing Profiles Relative module activation levels
Relative muscle weightings
1
0 1
0 TA
MG
VM
RF
MH
Module SCI-1a
Module SCI-2a
0
GM
20
40
60
80
100
80
100
Gait cycle (%)
B
1
Module SCI-1b
Relative module activation levels
0 1
Relative muscle weightings
Fig. 4. Muscle module weightings and timing profiles identified during treadmill walking in children with ISCIs. A, left: muscle module weights for both lower extremities in 2 children with ISCIs. Right: activation timing profiles represent the relative activation of the 2 modules for the right and left legs across the gait cycle (0 –100%). B, left: muscle module weights for both lower extremities of a child with ISCI who used 4 modules during treadmill walking. Right: activation timing profiles for both lower extremities of this child are displayed. Muscle weights for the TA, MG, VM, RF, MH, and GM muscles are represented.
0 1
Module SCI-2b
Module SCI-3b
0 1
Module SCI-4b
0 TA
MG
VM
RF
MH
GM
0
20
40
60
Gait cycle (%)
modules to account for muscle activation in children with ISCIs. The children with ISCIs were provided partial body weight support, physical assistance, and cueing to perform treadmill walking in a manner consistent with unimpaired walking. Thus locomotor-specific afferent input pertaining to lower extremity loading, limb kinematics, stepping speed, and reciprocal arm movements was enhanced during treadmill walking (Behrman and Harkema 2007) compared with afferent input during other tasks. This ensemble of task-specific sensory inputs regulates neuromuscular activation during walking (Maegele et al. 2002) and may have contributed to the activation of additional modules and a more complex locomotor output. This was most apparent in the child (SCI-6) who exhibited little activation in muscles below his injury yet required four modules to account for muscle activation during treadmill walking. This child had a lower extremity motor score of 0/50 and tests of voluntary movement indicating that he only could perform slight contractions of his hip flexor
muscles and slight toe movements. During all locomotor tasks, he required nearly full assistance to complete the tasks. Based on these factors, his muscle activation during treadmill walking may reflect the influence of task-specific afferent input on spinal centers below his spinal cord lesion (Dietz and Harkema 2004; Harkema 2008; Maegele et al. 2002). It is intriguing that some characteristics of this child’s modular output were relatively consistent with healthy modular control, whereas some features were altered. For instance, module SCI-2c (Fig. 4B) consisted primarily of MG activation, which is similar to module C-2a (healthy child; Fig. 2). Module SCI-2c, however, had a timing profile that was not consistent with modules identified in controls. The timing profile (module SCI-2c, Fig. 4B) did not have clear peaks of activation and was asymmetric across the right and left lower extremities. In contrast to treadmill walking, children with ISCIs walked overground at slower speeds, relied on a reverse rolling walker, and used alternative movement strategies to advance their limb
J Neurophysiol • doi:10.1152/jn.00676.2012 • www.jn.org
MODULAR CONTROL OF LOCOMOTION IN CHILDREN
during each step. Use of the rolling walker partially unloaded the lower extremities and transferred weight from the legs to the arms. During overground walking, therefore, the afferent input was less consistent with healthy coordinated walking compared with treadmill walking. This altered afferent input associated with an abnormal walking pattern and use of an assistive device may have distorted the motor activation during overground walking and reduced the number of modules required (Beres-Jones and Harkema 2004; Maegele et al. 2002; Phadke et al. 2007; Visintin and Barbeau 1994). Methodological Limitations The outcomes from this study may be influenced by methodological factors such as the number of subjects, injury severity, differences in the task conditions (e.g., use of a walker) across the two groups of children, and the number of lower extremity EMGs. We studied modular control in a small set of healthy children and children with ISCIs. Although our results are consistent with prior studies of modular control in adults and adults with neurological injuries, the findings may apply to a specific population of children with ISCIs. Children with spinal cord injuries (complete and incomplete) represent ⬃10% of the population of individuals with spinal cord injuries (Vitale et al. 2006). Our cohort of children with ISCIs, therefore, represents a subset of the population of children with spinal cord injuries. Furthermore, the children with ISCIs who participated in this study had severe, chronic injuries. Injury severity was evaluated on the basis of the Lower Extremity Motor Score or the amount of volitional, isolated lower extremity joint movement and strength (Table 1). Thus our findings may reflect neuromuscular control in a limited population of children with severe, chronic ISCIs. To compare similar rhythmic, reciprocal movements in the two groups of children, physical assistance was provided to the children with ISCIs and the use of an assistive device was required to enable independent ambulation overground. These differences in task conditions may have affected the modular organization of muscle activation and influenced the results of our study. Thus an alternative interpretation of the data may be that differences in modular control between the two groups are attributed to the differences in task conditions (i.e., assistive device use and manual assistance). Although these factors were not elucidated in children with ISCIs, comparisons of muscle activation in ambulatory adults with ISCIs during treadmill walking indicate that the patterns of muscle activation are generally unchanged when manual assistance is provided (Domingo et al. 2007). Moreover, studies examining the effect of various load perturbations (Cheung et al. 2009) and biomechanical constraints (Torres-Oviedo and Ting 2010) indicate that modular control remains consistent under various task conditions, suggesting a fundamental neural control strategy (Ting and McKay 2007). It is unclear how the nervous system develops new motor modules and at what threshold the task conditions require alterations in the neural control strategy (Cheung et al. 2012). This may be particularly relevant when the nervous system is not fully developed or injured, such as in the case of children with ISCIs (Torres-Oviedo and Ting 2010). A control group of children with fully intact central nervous system function, with task conditions specifically matched, (i.e., device use and
1423
manual assistance) may be particularly useful in expounding these factors. The number of lower extremity EMGs that were recorded also could influence the outcomes of this study. Indeed, a greater number of EMGs would further enhance our understanding of neuromuscular control and allow for more direct comparisons with previous studies of modular output (Bowden et al. 2010; Clark et al. 2010). We would not, however, expect the overall results of this study to be altered by a greater number of recordings. Because the same number of EMGs (6, bilateral lower extremity muscles) was recorded in the controls and children with ISCIs, we would expect the relative proportion of modules in the two groups to remain consistent even if the number of EMGs was increased. Additionally, the six bilateral lower extremity EMGs recorded activation in key muscles associated with locomotor control and previously identified to be distributed across each of the four modules activated during walking (Clark et al. 2010; Gizzi et al. 2012). Although additional recordings of lower extremity and trunk muscles can provide greater insights into synergistic muscle activation, a fundamental modular organization of muscle activation can be identified from a limited number of recordings (Gizzi et al. 2011). Gizzi and colleagues tested the effect of recording from a smaller set of muscles by comparing the results of their factorization based on 16 bilateral EMGS to their results from 7 bilateral EMGs. In both instances, four modules were required to account for the recorded muscle activation. The modular organization exhibited by each child with ISCI likely was influenced by factors that could not feasibly be controlled, including those pertaining to the child’s injury (e.g., etiology, age at the time of injury), motor experiences before and after injury, and rehabilitation experiences (Edgerton 2004). Indeed, the children with ISCIs had diverse injuries and motor experiences. For instance, two of five children were injured as infants and never developed walking before injury. Two children were injured secondary to traumatic accidents and a third child had an ISCI caused by a surgical resection of a spinal tumor. Of the two children who walked overground with a rolling walker, one was injured as an infant and had not developed walking skills before injury, and the other had a traumatic injury at 3.5 years and was nonambulatory for 16 mo after injury. Interestingly, both children gained walking function after several months of locomotor training (Behrman et al. 2008). Moreover, both children required two modules to account for the activation in each of their lower extremities (n ⫽ 4 lower extremities, each required 2 modules) (Fig. 4A). Therefore, despite a small sample size, the diversity of injuries and experiences among the children may indicate that the findings of reduced modular control in the children with ISCIs and similar modular control across tasks may be particularly meaningful relative to the effect of pediatric spinal cord injury on fundamental control mechanisms. Clinical Application Identification of fewer modules required to account for the muscle activation across locomotor tasks in children with ISCIs provides evidence of the effect of ISCI on neuromuscular control mechanisms (Safavynia et al. 2011). Identifying underlying mechanisms associated with locomotor control is
J Neurophysiol • doi:10.1152/jn.00676.2012 • www.jn.org
1424
MODULAR CONTROL OF LOCOMOTION IN CHILDREN
critical for the development of rehabilitation interventions designed to restore walking and locomotor function after pediatric-onset ISCI. Furthermore, the use of shared control strategies across varied locomotor tasks suggests that rehabilitation interventions, such as locomotor training, that activate spinal neural networks (Edgerton et al. 2004) may have benefits that extend to a variety of locomotor tasks (Stoloff et al. 2007). ACKNOWLEDGMENTS We thank and acknowledge the assistance of the engineering support staff of the Human Motor Performance Laboratory, located at the Malcom Randall Veterans Affairs Medical Center Brain Rehabilitation Research Center, as well as Dr. Evangelos Christou, PhD, for constructive feedback on earlier drafts of this manuscript. We thank the volunteers, students, and families that participated in this research. GRANTS This work was supported by Brooks Rehabilitation, the Florida Department of Health Brain & Spinal Cord Injury Program, the Craig H. Neilsen Foundation, the McKnight Brain Institute Rehabilitation Research Fund, and the University of Florida Clinical Translational Science Institute, as well as National Institutes of Health Grants K01 HD0134801 and TL1 RR029889. DISCLOSURES No conflicts of interest, financial or otherwise, are declared by the authors. AUTHOR CONTRIBUTIONS E.J.F., S.A.K., D.R.H., D.J.C., and A.L.B. conception and design of research; E.J.F., N.J.T., and A.L.B. performed experiments; E.J.F. and C.G. analyzed data; E.J.F., S.A.K., D.R.H., D.J.C., and A.L.B. interpreted results of experiments; E.J.F. prepared figures; E.J.F. drafted manuscript; E.J.F., N.J.T., S.A.K., D.R.H., D.J.C., C.G., and A.L.B. edited and revised manuscript; E.J.F., N.J.T., S.A.K., D.R.H., D.J.C., C.G., and A.L.B. approved final version of manuscript. REFERENCES American Spinal Injury Association. Standards for Neurological Classification of Spinal Cord Injury. Chicago, IL: American Spinal Injury Association, 2006. Behrman AL, Harkema SJ. Locomotor training after human spinal cord injury: a series of case studies. Phys Ther 80: 688 –700, 2000. Behrman AL, Harkema SJ. Physical rehabilitation as an agent for recovery after spinal cord injury. Phys Med Rehabil Clin N Am 18: 183–202, 2007. Behrman AL, Nair PM, Bowden MG, Dauser RC, Herget BR, Martin JB, Phadke CP, Reier PJ, Senesac CR, Thompson FJ, Howland DR. Locomotor training restores walking in a nonambulatory child with chronic, severe, incomplete cervical spinal cord injury. Phys Ther 88: 580 –590, 2008. Beres-Jones JA, Harkema SJ. The human spinal cord interprets velocitydependent afferent input during stepping. Brain 127: 2232–2246, 2004. Berkowitz A. Physiology and morphology of shared and specialized spinal interneurons for locomotion and scratching. J Neurophysiol 99: 2887–2901, 2008. Bizzi E, Cheung VC, d’Avella A, Saltiel P, Tresch M. Combining modules for movement. Brain Res Rev 57: 125–133, 2008. Bizzi E, Mussa-Ivaldi FA, Giszter S. Computations underlying the execution of movement: a biological perspective. Science 253: 287–291, 1991. Bizzi E, Tresch MC, Saltiel P, d’Avella A. New perspectives on spinal motor systems. Nat Rev Neurosci 1: 101–108, 2000. Bowden MG, Clark DJ, Kautz SA. Evaluation of abnormal synergy patterns poststroke: relationship of the Fugl-Meyer Assessment to hemiparetic locomotion. Neurorehabil Neural Repair 24: 328 –337, 2010. Bregman BS, Goldberger ME. Infant lesion effect: II. Sparing and recovery of function after spinal cord damage in newborn and adult cats. Brain Res 285: 119 –135, 1983.
Calancie B, Needham-Shropshire B, Jacobs P, Willer K, Zych G, Green BA. Involuntary stepping after chronic spinal cord injury. Evidence for a central rhythm generator for locomotion in man. Brain 117: 1143–1159, 1994. Cheung VC, Turolla A, Agostini M, Silvoni S, Bennis C, Kasi P, Paganoni S, Bonato P, Bizzi E. Muscle synergy patterns as physiological markers of motor cortical damage. Proc Natl Acad Sci USA 109: 14652–14656, 2012. Cheung VC, d’Avella A, Bizzi E. Adjustments of motor pattern for load compensation via modulated activations of muscle synergies during natural behaviors. J Neurophysiol 101: 1235–1257, 2009. Cheung VC, d’Avella A, Tresch MC, Bizzi E. Central and sensory contributions to the activation and organization of muscle synergies during natural motor behaviors. J Neurosci 25: 6419 – 6434, 2005. Clark DJ, Ting LH, Zajac FE, Neptune RR, Kautz SA. Merging of healthy motor modules predicts reduced locomotor performance and muscle coordination complexity post-stroke. J Neurophysiol 103: 844 – 857, 2010. Cohen J. Statistical power analysis for the behavioral sciences (2nd ed.). Hillsdale, NJ: Lawrence Earlbaum Associates, 1988. Damiano DL, DeJong SL. A systematic review of the effectiveness of treadmill training and body weight support in pediatric rehabilitation. J Neurol Phys Ther 33: 27– 44, 2009. d’Avella A, Saltiel P, Bizzi E. Combinations of muscle synergies in the construction of a natural motor behavior. Nat Neurosci 6: 300 –308, 2003. Dietz V. Spinal cord pattern generators for locomotion. Clin Neurophysiol 114: 1379 –1389, 2003. Dietz V, Harkema SJ. Locomotor activity in spinal cord-injured persons. J Appl Physiol 96: 1954 –1960, 2004. Dietz V, Muller R, Colombo G. Locomotor activity in spinal man: significance of afferent input from joint and load receptors. Brain 125: 2626 –2634, 2002. Dimitrijevic MR, Gerasimenko Y, Pinter MM. Evidence for a spinal central pattern generator in humans. Ann NY Acad Sci 860: 360 –376, 1998. Dobkin BH, Harkema S, Requejo P, Edgerton VR. Modulation of locomotor-like EMG activity in subjects with complete and incomplete spinal cord injury. J Neurol Rehabil 9: 183–190, 1995. Domingo A, Sawicki GS, Ferris DP. Kinematics and muscle activity of individuals with incomplete spinal cord injury during treadmill stepping with and without manual assistance. J Neuroeng Rehabil 4: 32, 2007. Dominici N, Ivanenko YP, Cappellini G, d’Avella A, Mondi V, Cicchese M, Fabiano A, Silei T, Di Paolo A, Giannini C, Poppele RE, Lacquaniti F. Locomotor primitives in newborn babies and their development. Science 334: 997–999, 2011. Earhart GM, Stein PS. Step, swim, and scratch motor patterns in the turtle. J Neurophysiol 84: 2181–2190, 2000. Edgerton VR, Tillakaratne NJ, Bigbee AJ, de Leon RD, Roy RR. Plasticity of the spinal neural circuitry after injury. Annu Rev Neurosci 27: 145–167, 2004. Ferris DP, Gordon KE, Beres-Jones JA, Harkema SJ. Muscle activation during unilateral stepping occurs in the nonstepping limb of humans with clinically complete spinal cord injury. Spinal Cord 42: 14 –23, 2004. Forssberg H, Grillner S, Halbertsma J, Rossignol S. The locomotion of the low spinal cat. II. Interlimb coordination. Acta Physiol Scand 108: 283–295, 1980. Fox EJ, Kautz SA, Day KV, Suter SP, Clark DJ, Howland DR, Behrman AL. Mechanisms of walking recovery following locomotor training in adults with incomplete spinal cord injury. Program 276.12. 2011 Neuroscience Meeting Planner. Washington, DC: Society for Neuroscience, 2011. Fox EJ, Tester NJ, Phadke CP, Nair PM, Senesac CR, Howland DR, Behrman AL. Ongoing walking recovery 2 years after locomotor training in a child with severe incomplete spinal cord injury. Phys Ther 90: 793– 802, 2010. Gentner R, Classen J. Modular organization of finger movements by the human central nervous system. Neuron 52: 731–742, 2006. Gizzi L, Nielsen JF, Felici F, Ivanenko YP, Farina D. Impulses of activation but not motor modules are preserved in the locomotion of subacute stroke patients. J Neurophysiol 106: 202–210, 2011. Gizzi L, Nielsen JF, Felici F, Moreno J, Pons JL, Farina D. Motor modules in robot-aided walking. J Neuroeng Rehabil 9: 76, 2012. Grillner S. Interaction between central and peripheral mechanisms in the control of locomotion. Prog Brain Res 50: 227–235, 1979. Grillner S, Wallen P, Saitoh K, Kozlov A, Robertson B. Neural bases of goal-directed locomotion in vertebrates–an overview. Brain Res Rev 57: 2–12, 2008.
J Neurophysiol • doi:10.1152/jn.00676.2012 • www.jn.org
MODULAR CONTROL OF LOCOMOTION IN CHILDREN Grillner S, Zangger P. How detailed is the central pattern generation for locomotion? Brain Res 88: 367–371, 1975. Harkema SJ. Plasticity of interneuronal networks of the functionally isolated human spinal cord. Brain Res Rev 57: 255–264, 2008. Harkema SJ, Hurley SL, Patel UK, Requejo PS, Dobkin BH, Edgerton VR. Human lumbosacral spinal cord interprets loading during stepping. J Neurophysiol 77: 797– 811, 1997. Hart CB, Giszter SF. Modular premotor drives and unit bursts as primitives for frog motor behaviors. J Neurosci 24: 5269 –5282, 2004. Hart CB, Giszter SF. A neural basis for motor primitives in the spinal cord. J Neurosci 30: 1322–1336, 2010. Hayes HB, VanHiel LR, Chvatal SA, Ting LH, Tansey KE, Trumbower RD. Modularity of muscle activity during robot-assisted locomotion in persons with incomplete spinal cord injury. Program 808.13. 2011 Neuroscience Meeting Planner. Washington, DC: Society for Neuroscience, 2011. Holdefer RN, Miller LE. Primary motor cortical neurons encode functional muscle synergies. Exp Brain Res 146: 233–243, 2002. Ivanenko YP, Cappellini G, Dominici N, Poppele RE, Lacquaniti F. Coordination of locomotion with voluntary movements in humans. J Neurosci 25: 7238 –7253, 2005. Ivanenko YP, Grasso R, Zago M, Molinari M, Scivoletto G, Castellano V, Macellari V, Lacquaniti F. Temporal components of the motor patterns expressed by the human spinal cord reflect foot kinematics. J Neurophysiol 90: 3555–3565, 2003. Ivanenko YP, Poppele RE, Lacquaniti F. Five basic muscle activation patterns account for muscle activity during human locomotion. J Physiol 556: 267–282, 2004. Kadaba MP, Ramakrishnan HK, Wootten ME, Gainey J, Gorton G, Cochran GV. Repeatability of kinematic, kinetic, and electromyographic data in normal adult gait. J Orthop Res 7: 849 – 860, 1989. Kargo WJ, Giszter SF. Individual premotor drive pulses, not time-varying synergies, are the units of adjustment for limb trajectories constructed in spinal cord. J Neurosci 28: 2409 –2425, 2008. Kargo WJ, Giszter SF. Rapid correction of aimed movements by summation of force-field primitives. J Neurosci 20: 409 – 426, 2000. Kozlov A, Huss M, Lansner A, Kotaleski JH, Grillner S. Simple cellular and network control principles govern complex patterns of motor behavior. Proc Natl Acad Sci USA 106: 20027–20032, 2009. Lamb T, Yang JF. Could different directions of infant stepping be controlled by the same locomotor central pattern generator? J Neurophysiol 83: 2814 –2824, 2000. Lee D, Seung H. Learning the parts of objects by non-negative matrix factorization. Nature 788 –791, 1999. Maegele M, Muller S, Wernig A, Edgerton VR, Harkema SJ. Recruitment of spinal motor pools during voluntary movements versus stepping after human spinal cord injury. J Neurotrauma 19: 1217–1229, 2002. Marder E, Bucher D. Central pattern generators and the control of rhythmic movements. Curr Biol 11: R986 –996, 2001. McGowan CP, Neptune RR, Clark DJ, Kautz SA. Modular control of human walking: adaptations to altered mechanical demands. J Biomech 43: 412– 419, 2010. Mortin L, Stein P. Spinal cord segments containing key elements of the central pattern generators for three forms of scratch reflex in the turtle. J Neurosci 9: 2285–2296, 1989. Mussa-Ivaldi FA, Giszter SF, Bizzi E. Linear combinations of primitives in vertebrate motor control. Proc Natl Acad Sci USA 91: 7534 –7538, 1994. Nadeau S, Jacquemin G, Fournier C, Lamarre Y, Rossignol S. Spontaneous motor rhythms of the back and legs in a patient with a complete spinal cord transection. Neurorehabil Neural Repair 24: 377–383, 2010.
1425
Neptune RR, Clark DJ, Kautz SA. Modular control of human walking: a simulation study. J Biomech 42: 1282–1287, 2009. Patrick SK, Noah JA, Yang JF. Interlimb coordination in human crawling reveals similarities in development and neural control with quadrupeds. J Neurophysiol 101: 603– 613, 2009. Petersen TH, Kliim-Due M, Farmer SF, Nielsen JB. Childhood development of common drive to a human leg muscle during ankle dorsiflexion and gait. J Physiol 588: 4387– 4400, 2010. Phadke CP, Wu SS, Thompson FJ, Behrman AL. Comparison of soleus H-reflex modulation after incomplete spinal cord injury in 2 walking environments: treadmill with body weight support and overground. Arch Phys Med Rehabil 88: 1606 –1613, 2007. Roh J, Cheung VC, Bizzi E. Modules in the brain stem and spinal cord underlying motor behaviors. J Neurophysiol 106: 1363–1378, 2011. Rossignol S, Dubuc R, Gossard JP. Dynamic sensorimotor interactions in locomotion. Physiol Rev 86: 89 –154, 2006. Safavynia SA, Torres-Oviedo G, Ting LH. Muscle synergies: implications for clinical evaluation and rehabilitation of movement. Top Spinal Cord Inj Rehabil 17: 16 –24, 2011. Stoloff RH, Zehr EP, Ferris DP. Recumbent stepping has similar but simpler neural control compared to walking. Exp Brain Res 178: 427– 438, 2007. Sutherland D, Olshen R, Cooper L, Woo S. The development of mature gait. J Bone Joint Surg Am 62: 336 –353, 1980. Ting LH. Dimensional reduction in sensorimotor systems: a framework for understanding muscle coordination of posture. Prog Brain Res 165: 299 – 321, 2007. Ting LH, Macpherson JM. A limited set of muscle synergies for force control during a postural task. J Neurophysiol 93: 609 – 613, 2005. Ting LT, McKay. Neuromechanics of muscle synergies for posture and movement. Curr Opin Neurobiol 17: 622–28, 2007. Torres-Oviedo G, Ting LH. Subject-specific muscle synergies in human balance control are consistent across different biomechanical contexts. J Neurophysiol 103: 3084 –3098, 2010. Torres-Oviedo G, Macpherson JM, Ting LH. Muscle synergy organization is robust across a variety of postural perturbations. J Neurophysiol 96: 1530 –1546, 2006. Tresch MC, Saltiel P, Bizzi E. The construction of movement by the spinal cord. Nat Neurosci 2: 162–167, 1999. Visintin M, Barbeau H. The effects of parallel bars, body weight support and speed on the modulation of the locomotor pattern of spastic paretic gait. A preliminary communication. Paraplegia 32: 540 –553, 1994. Vitale MG, Goss JM, Matsumoto H, Roye DP. Epidemiology of pediatric spinal cord injury in the United States years 1997–2000. J Pediatr Orthop 26: 745–749, 2006. Vogel LC, Lubicky JP. Ambulation in children and adolescents with spinal cord injuries. J Pediatr Orthop 15: 510 –516, 1995. Wannier T, Bastiaanse C, Colombo G, Dietz V. Arm to leg coordination in humans during walking, creeping and swimming activities. Exp Brain Res 141: 375–379, 2001. Winter DA, Fuglevand AJ, Archer SE. Crosstalk in surface electromyography: theoretical and practical estimates. J Electromyogr Kinesiol 4: 15–26, 1994. Zehr EP. Neural control of rhythmic human movement: the common core hypothesis. Exerc Sport Sci Rev 33: 54 – 60, 2005. Zehr EP, Balter JE, Ferris DP, Hundza SR, Loadman PM, Stoloff RH. Neural regulation of rhythmic arm and leg movement is conserved across human locomotor tasks. J Physiol 582: 209 –227, 2007.
J Neurophysiol • doi:10.1152/jn.00676.2012 • www.jn.org